Effects of different cancer-directed therapies on mortality of patients with stage I pulmonary large cell neuroendocrine carcinoma: a retrospective cohort study based on the SEER database.
{"title":"Effects of different cancer-directed therapies on mortality of patients with stage I pulmonary large cell neuroendocrine carcinoma: a retrospective cohort study based on the SEER database.","authors":"Shijun Chen, Mohan Weng, Yanru Jiang, Tingting Li, Qicai Li, Chengling Zhao","doi":"10.21037/tcr-2024-2551","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pulmonary large cell neuroendocrine carcinoma (LCNEC) is a rare subtype of lung tumors with the characteristics of both small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC), but has a worse prognosis. At present, there is no consensus on the optimal clinical therapy of LCNEC. This study aims to explore the effects of different cancer-directed therapies on mortality of stage I LCNEC patients.</p><p><strong>Methods: </strong>Data of this retrospective cohort study were extracted from the Surveillance Epidemiology and End Results (SEER) 2004-2015. Surgery, radiotherapy and their combination therapy were considered as cancer-directed therapy. The univariate and multivariate competing-risks model and COX proportional hazard model were utilized to explore the effect of different cancer-directed therapies on the all-cause mortality and cancer-species mortality of stage I LCNEC patients respectively and described as hazard ratios (HRs) and 95% confidence intervals (CIs). Subgroup analysis was conducted to further evaluate the effect.</p><p><strong>Results: </strong>A total of 469 LCNEC patients were included, with 326 deaths recorded by December 31, 2015. Significant differences were observed between survivors and deceased patients in age, year of diagnosis, number of lymph nodes, type of surgery, use of radiation, combined treatments, and cancer-specific mortality. In the fully adjusted model, sublobectomy alone showed a lower HR compared to other treatments. No significant difference of mortality was found between patients who underwent lobectomy alone and sublobectomy alone. No statistically significant differences in mortality were found between patients receiving radiation combined with sublobectomy or lobectomy and those receiving sublobectomy alone. In patients younger than 65 years, combined radiation and other treatments increased mortality compared to sublobectomy alone. In patients older than 65 years, radiation or extended resection also increased mortality. Sublobectomy was the most favorable treatment for female patients and those classified as American Joint Committee on Cancer (AJCC) T1. Male patients who underwent lobectomy exhibited better prognoses. Extended resection or radiation alone or combined with other treatment in patients with cancer laterality increased mortality risk.</p><p><strong>Conclusions: </strong>Sublobectomy alone appears to be an effective treatment option for stage I LCNEC patients, outperforming combined therapies involving radiation and resection. Radiation therapy requires careful consideration, as it showed no significant mortality benefit when used alone or combined with sublobectomy or lobectomy. Lobectomy provided better prognoses for male patients, and radiation or extended resection offered limited advantages. And these findings need to be further confirmed by large-scale randomized controlled trails in the future.</p>","PeriodicalId":23216,"journal":{"name":"Translational cancer research","volume":"14 8","pages":"4906-4919"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12432775/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational cancer research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tcr-2024-2551","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/11 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pulmonary large cell neuroendocrine carcinoma (LCNEC) is a rare subtype of lung tumors with the characteristics of both small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC), but has a worse prognosis. At present, there is no consensus on the optimal clinical therapy of LCNEC. This study aims to explore the effects of different cancer-directed therapies on mortality of stage I LCNEC patients.
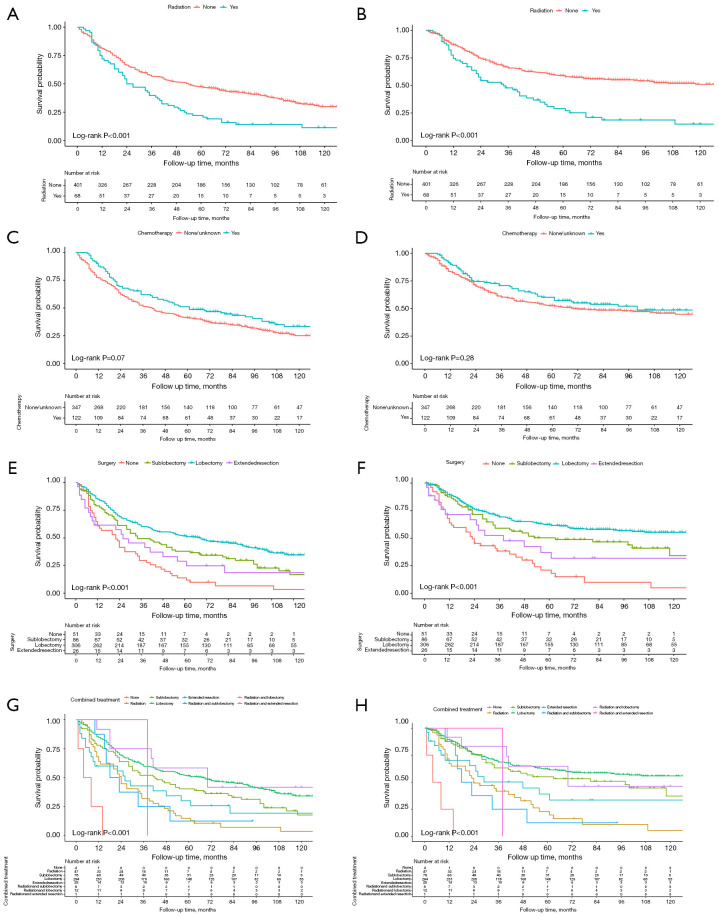
Methods: Data of this retrospective cohort study were extracted from the Surveillance Epidemiology and End Results (SEER) 2004-2015. Surgery, radiotherapy and their combination therapy were considered as cancer-directed therapy. The univariate and multivariate competing-risks model and COX proportional hazard model were utilized to explore the effect of different cancer-directed therapies on the all-cause mortality and cancer-species mortality of stage I LCNEC patients respectively and described as hazard ratios (HRs) and 95% confidence intervals (CIs). Subgroup analysis was conducted to further evaluate the effect.
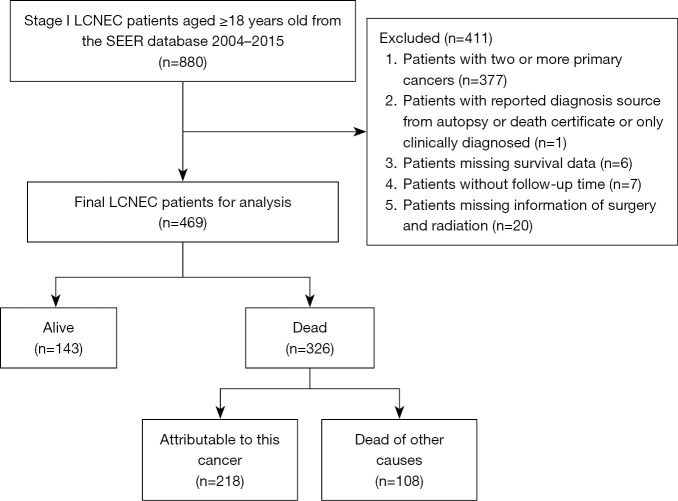
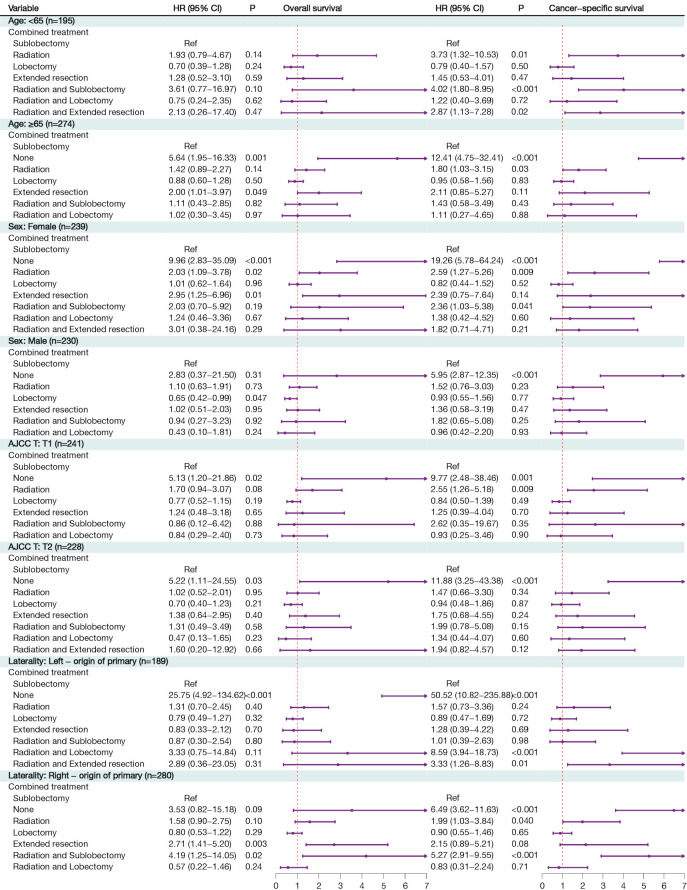
Results: A total of 469 LCNEC patients were included, with 326 deaths recorded by December 31, 2015. Significant differences were observed between survivors and deceased patients in age, year of diagnosis, number of lymph nodes, type of surgery, use of radiation, combined treatments, and cancer-specific mortality. In the fully adjusted model, sublobectomy alone showed a lower HR compared to other treatments. No significant difference of mortality was found between patients who underwent lobectomy alone and sublobectomy alone. No statistically significant differences in mortality were found between patients receiving radiation combined with sublobectomy or lobectomy and those receiving sublobectomy alone. In patients younger than 65 years, combined radiation and other treatments increased mortality compared to sublobectomy alone. In patients older than 65 years, radiation or extended resection also increased mortality. Sublobectomy was the most favorable treatment for female patients and those classified as American Joint Committee on Cancer (AJCC) T1. Male patients who underwent lobectomy exhibited better prognoses. Extended resection or radiation alone or combined with other treatment in patients with cancer laterality increased mortality risk.
Conclusions: Sublobectomy alone appears to be an effective treatment option for stage I LCNEC patients, outperforming combined therapies involving radiation and resection. Radiation therapy requires careful consideration, as it showed no significant mortality benefit when used alone or combined with sublobectomy or lobectomy. Lobectomy provided better prognoses for male patients, and radiation or extended resection offered limited advantages. And these findings need to be further confirmed by large-scale randomized controlled trails in the future.
期刊介绍:
Translational Cancer Research (Transl Cancer Res TCR; Print ISSN: 2218-676X; Online ISSN 2219-6803; http://tcr.amegroups.com/) is an Open Access, peer-reviewed journal, indexed in Science Citation Index Expanded (SCIE). TCR publishes laboratory studies of novel therapeutic interventions as well as clinical trials which evaluate new treatment paradigms for cancer; results of novel research investigations which bridge the laboratory and clinical settings including risk assessment, cellular and molecular characterization, prevention, detection, diagnosis and treatment of human cancers with the overall goal of improving the clinical care of cancer patients. The focus of TCR is original, peer-reviewed, science-based research that successfully advances clinical medicine toward the goal of improving patients'' quality of life. The editors and an international advisory group of scientists and clinician-scientists as well as other experts will hold TCR articles to the high-quality standards. We accept Original Articles as well as Review Articles, Editorials and Brief Articles.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


