{"title":"Predicting Amyotrophic Lateral Sclerosis Mortality With Machine Learning in Diverse Patient Databases.","authors":"Ling Guo, Ian Qian Xu, Sonakshi Nag, Jing Xu, Josiah Chai, Zachary Simmons, Savitha Ramasamy, Crystal Jing Jing Yeo","doi":"10.1002/mus.28487","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Predicting mortality in Amyotrophic Lateral Sclerosis (ALS) guides personalized care and clinical trial optimization. Existing statistical and machine learning models often rely on baseline or diagnosis visit data, assume fixed predictor-survival relationships, lack validation in non-Western populations, and depend on features like genetic tests and imaging not routinely available. This study developed ALS mortality prediction models that address these limitations.</p><p><strong>Methods: </strong>We trained Royston-Parmar and eXtreme Gradient Boosting models on the PRO-ACT database for 6- and 12-month mortality predictions. Each visit was labeled positive (for death) if death occurred within 6 or 12 months, negative if survival was confirmed beyond that, and excluded if follow-up was insufficient, assuming patients were alive up to their last recorded visit. Models were validated on independent datasets from the North American Celecoxib trial and a Singapore ALS clinic population. Feature importance and the impact of reducing predictors on performance were evaluated.</p><p><strong>Results: </strong>Models predicted mortality from any clinical visit with area under the curve (AUC) of 0.768-0.819, rising to 0.865 for 12-month prediction using 3-month windows. Albumin was the top predictor, reflecting nutritional and inflammatory status. Other key predictors included ALS Functional Rating Scale-Revised slope, limb onset, absolute basophil count, forced vital capacity, bicarbonate, body mass index, and respiratory rate. Models maintained robust performance on the independent datasets and after reducing inputs to seven key predictors.</p><p><strong>Discussion: </strong>These visit-agnostic models, validated across diverse populations, identify key prognostic features and demonstrate the potential of predictive modeling to enhance ALS care and trial design.</p>","PeriodicalId":18968,"journal":{"name":"Muscle & Nerve","volume":"72 4","pages":"653-661"},"PeriodicalIF":3.1000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12435129/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Muscle & Nerve","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/mus.28487","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/28 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Predicting mortality in Amyotrophic Lateral Sclerosis (ALS) guides personalized care and clinical trial optimization. Existing statistical and machine learning models often rely on baseline or diagnosis visit data, assume fixed predictor-survival relationships, lack validation in non-Western populations, and depend on features like genetic tests and imaging not routinely available. This study developed ALS mortality prediction models that address these limitations.
Methods: We trained Royston-Parmar and eXtreme Gradient Boosting models on the PRO-ACT database for 6- and 12-month mortality predictions. Each visit was labeled positive (for death) if death occurred within 6 or 12 months, negative if survival was confirmed beyond that, and excluded if follow-up was insufficient, assuming patients were alive up to their last recorded visit. Models were validated on independent datasets from the North American Celecoxib trial and a Singapore ALS clinic population. Feature importance and the impact of reducing predictors on performance were evaluated.
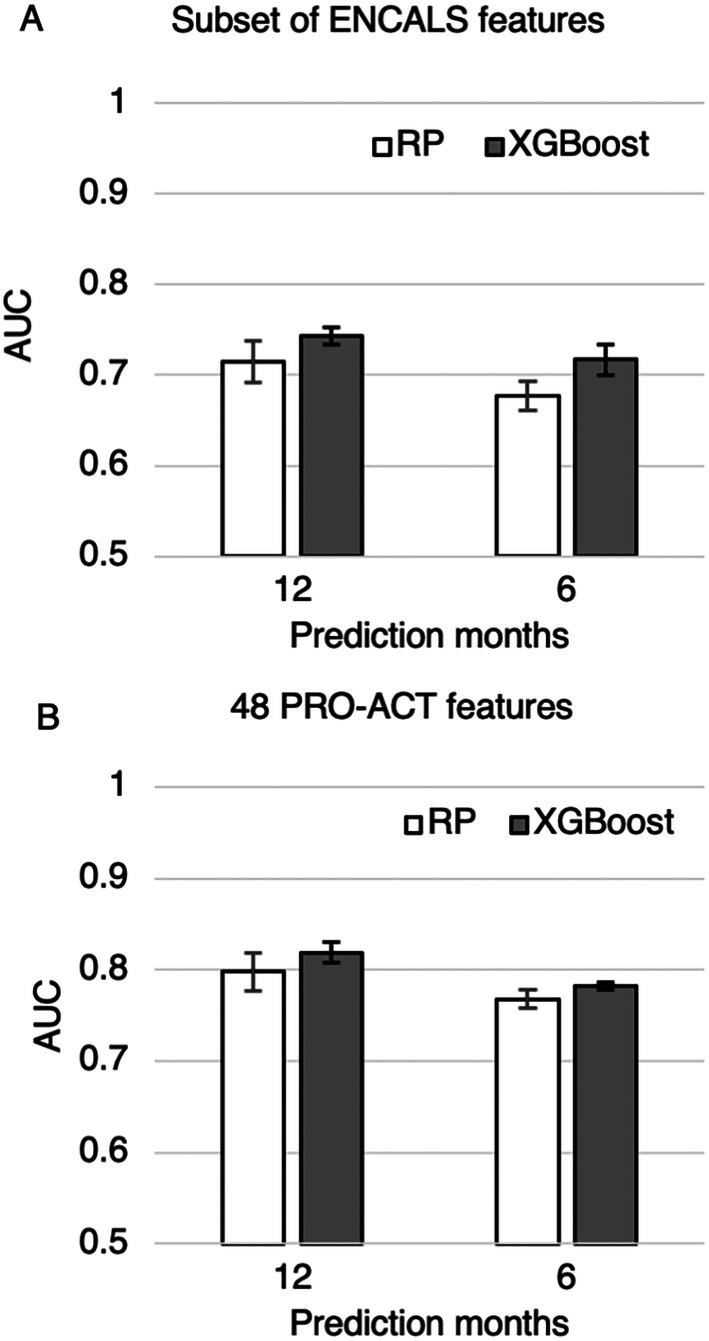
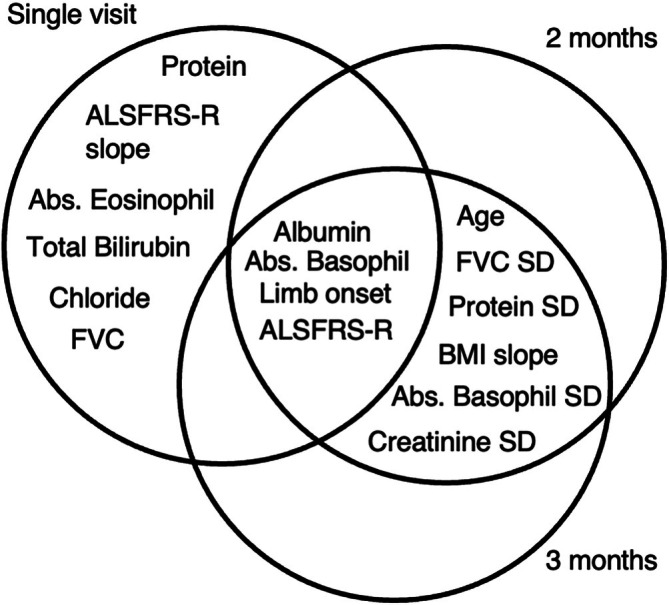
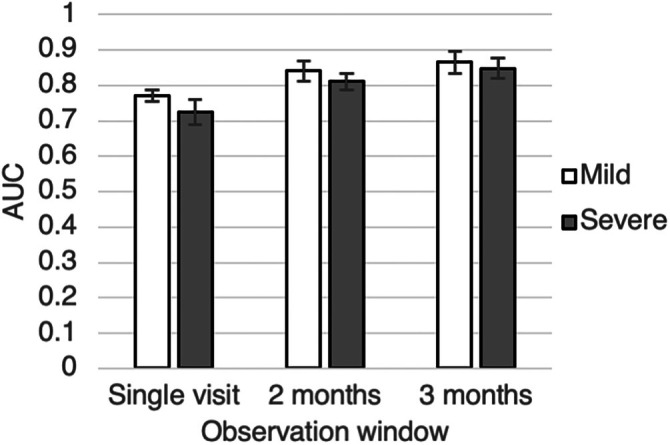
Results: Models predicted mortality from any clinical visit with area under the curve (AUC) of 0.768-0.819, rising to 0.865 for 12-month prediction using 3-month windows. Albumin was the top predictor, reflecting nutritional and inflammatory status. Other key predictors included ALS Functional Rating Scale-Revised slope, limb onset, absolute basophil count, forced vital capacity, bicarbonate, body mass index, and respiratory rate. Models maintained robust performance on the independent datasets and after reducing inputs to seven key predictors.
Discussion: These visit-agnostic models, validated across diverse populations, identify key prognostic features and demonstrate the potential of predictive modeling to enhance ALS care and trial design.
期刊介绍:
Muscle & Nerve is an international and interdisciplinary publication of original contributions, in both health and disease, concerning studies of the muscle, the neuromuscular junction, the peripheral motor, sensory and autonomic neurons, and the central nervous system where the behavior of the peripheral nervous system is clarified. Appearing monthly, Muscle & Nerve publishes clinical studies and clinically relevant research reports in the fields of anatomy, biochemistry, cell biology, electrophysiology and electrodiagnosis, epidemiology, genetics, immunology, pathology, pharmacology, physiology, toxicology, and virology. The Journal welcomes articles and reports on basic clinical electrophysiology and electrodiagnosis. We expedite some papers dealing with timely topics to keep up with the fast-moving pace of science, based on the referees'' recommendation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


