{"title":"Gender-specific differences in body mass index and cardiovascular risk adversely impact survival after aortic valve replacement.","authors":"Suvitesh Luthra, Hannah Masraf, Davorin Sef, David Thirukumaran, Szabolcs Miskolczi, Theodore Velissaris","doi":"10.21037/cdt-2025-113","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is a lack of evidence on association between gender specific differences in obesity and cardiovascular risk after isolated surgical aortic valve replacement (AVR) and its impact on outcomes and long-term survival. The aim of this study was to assess the impact of obesity on perioperative outcomes and long-term survival after isolated AVR.</p><p><strong>Methods: </strong>In this retrospective, single-centre study, we included all patients who underwent isolated AVR between April 2000 and December 2019 from the cardiac surgery database of the Southampton General Hospital (Patient Administration System, e-CAMIS, Yeadon, Leeds, UK). Patients with infective endocarditis, re-sternotomy, other concomitant cardiac procedures, homografts, autografts and emergency operations were excluded. Univariable regression analysis was performed to identify predictors of in-hospital mortality. Hazard ratios were calculated using a Cox proportional hazards model.</p><p><strong>Results: </strong>Total of 2,398 patients were included in the study and two groups of patients were compared: body mass index (BMI) 25-34.9 kg/m<sup>2</sup> (n=2,000) and BMI ≥35 kg/m<sup>2</sup> (n=398) based on sensitivity modelling. Actuarial survival was comparable across BMI groups at 12.5and 12.7 years for BMI 25-34.9 kg/m<sup>2</sup> and BMI ≥35 kg/m<sup>2</sup>, respectively (P=0.75 log-rank). Long-term survival was specifically worse for patients with high BMI and composite cardiovascular risk of hypertension, diabetes mellitus, and current smoking [hazard ratio (HR) 1.93, 95% confidence interval (CI): 1.45-2.58, P<0.001] and patients with moderate-to-severe patient prosthesis mismatch (PPM) (effective orifice areas index ≤0.85 cm<sup>2</sup>/m<sup>2</sup>) (HR 1.17 95% CI: 0.98-1.39, P=0.08). Median survival time for females was 11.5 years [interquartile range (IQR): 10.3-12.3 years] versus 14.2 years (IQR: 12.7-15.7 years) for males (log-rank P=0.006), although gender was not a significant predictor of long-term survival after adjusting for covariates. Moderate-severe PPM was associated with significantly worse survival in females (log-rank P<0.01), compared to males for whom this difference was not significant (log-rank P=0.21).</p><p><strong>Conclusions: </strong>Obesity with composite risk factors (hypertension, diabetes mellitus and active smoking) is associated with adverse survival. We did not observe gender-specific differences in long-term survival among specific BMI groups of patients.</p>","PeriodicalId":9592,"journal":{"name":"Cardiovascular diagnosis and therapy","volume":"15 4","pages":"770-780"},"PeriodicalIF":2.1000,"publicationDate":"2025-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12432612/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular diagnosis and therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/cdt-2025-113","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/26 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There is a lack of evidence on association between gender specific differences in obesity and cardiovascular risk after isolated surgical aortic valve replacement (AVR) and its impact on outcomes and long-term survival. The aim of this study was to assess the impact of obesity on perioperative outcomes and long-term survival after isolated AVR.
Methods: In this retrospective, single-centre study, we included all patients who underwent isolated AVR between April 2000 and December 2019 from the cardiac surgery database of the Southampton General Hospital (Patient Administration System, e-CAMIS, Yeadon, Leeds, UK). Patients with infective endocarditis, re-sternotomy, other concomitant cardiac procedures, homografts, autografts and emergency operations were excluded. Univariable regression analysis was performed to identify predictors of in-hospital mortality. Hazard ratios were calculated using a Cox proportional hazards model.
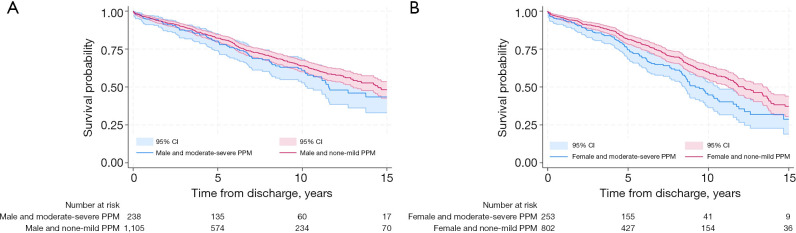
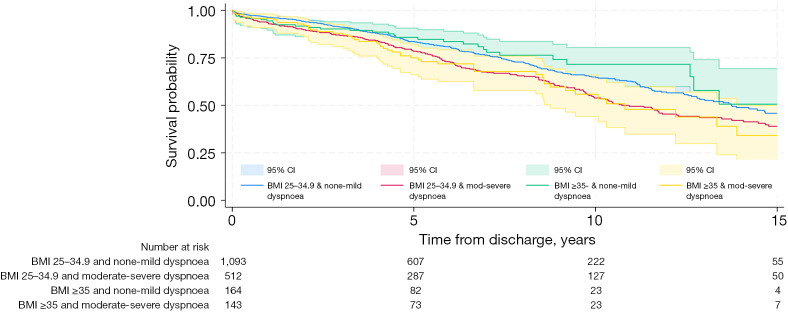
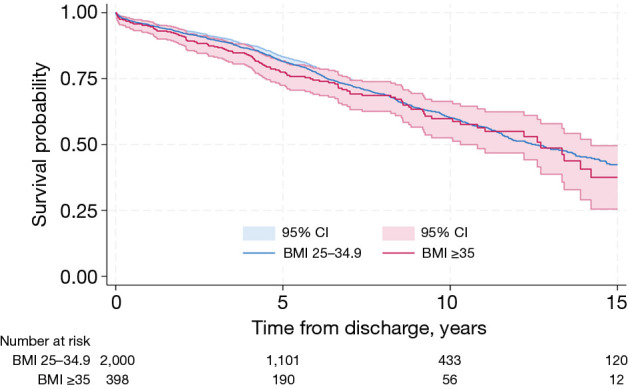
Results: Total of 2,398 patients were included in the study and two groups of patients were compared: body mass index (BMI) 25-34.9 kg/m2 (n=2,000) and BMI ≥35 kg/m2 (n=398) based on sensitivity modelling. Actuarial survival was comparable across BMI groups at 12.5and 12.7 years for BMI 25-34.9 kg/m2 and BMI ≥35 kg/m2, respectively (P=0.75 log-rank). Long-term survival was specifically worse for patients with high BMI and composite cardiovascular risk of hypertension, diabetes mellitus, and current smoking [hazard ratio (HR) 1.93, 95% confidence interval (CI): 1.45-2.58, P<0.001] and patients with moderate-to-severe patient prosthesis mismatch (PPM) (effective orifice areas index ≤0.85 cm2/m2) (HR 1.17 95% CI: 0.98-1.39, P=0.08). Median survival time for females was 11.5 years [interquartile range (IQR): 10.3-12.3 years] versus 14.2 years (IQR: 12.7-15.7 years) for males (log-rank P=0.006), although gender was not a significant predictor of long-term survival after adjusting for covariates. Moderate-severe PPM was associated with significantly worse survival in females (log-rank P<0.01), compared to males for whom this difference was not significant (log-rank P=0.21).
Conclusions: Obesity with composite risk factors (hypertension, diabetes mellitus and active smoking) is associated with adverse survival. We did not observe gender-specific differences in long-term survival among specific BMI groups of patients.
期刊介绍:
The journal ''Cardiovascular Diagnosis and Therapy'' (Print ISSN: 2223-3652; Online ISSN: 2223-3660) accepts basic and clinical science submissions related to Cardiovascular Medicine and Surgery. The mission of the journal is the rapid exchange of scientific information between clinicians and scientists worldwide. To reach this goal, the journal will focus on novel media, using a web-based, digital format in addition to traditional print-version. This includes on-line submission, review, publication, and distribution. The digital format will also allow submission of extensive supporting visual material, both images and video. The website www.thecdt.org will serve as the central hub and also allow posting of comments and on-line discussion. The web-site of the journal will be linked to a number of international web-sites (e.g. www.dxy.cn), which will significantly expand the distribution of its contents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


