Nooreena Yusop, Samsiah Mat, Ruslinda Mustafar, Muhammad Ishamuddin Ismail
{"title":"Fuzzy logic nursing tool for early acute kidney injury detection in surgical patients.","authors":"Nooreena Yusop, Samsiah Mat, Ruslinda Mustafar, Muhammad Ishamuddin Ismail","doi":"10.3389/fneph.2025.1624880","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute Kidney Injury (AKI) is a common yet preventable complication among surgical patients, contributing to increased morbidity, prolonged hospital stays, and higher healthcare costs. Early detection is critical; however, the absence of a standardized nursing-led risk assessment tool for AKI limits proactive intervention in clinical practice.</p><p><strong>Objective: </strong>This study aimed to develop and evaluate the Nursing Risk Assessment for Acute Kidney Injury tool, integrating the Fuzzy Logic Model (FLM) to enhance interpretive accuracy and improve nursing-led AKI risk detection and decision-making.</p><p><strong>Methods: </strong>A Design and Development Research (DDR) framework was employed in three phases. Phase 1 involved a needs analysis using a focus group discussion to explore the necessity of AKI assessment among surgical nurses. Phase 2 focused on tool development through expert consensus (surgeon, nephrologist, nursing academician, and experienced nurse) and evidence synthesis via a systematic literature review. In Phase 3, the Nursing Risk Assessment-AKI tool was evaluated through a quasi-experimental design at Hospital Canselor Tuanku Muhriz (HCTM), Kuala Lumpur, involving 75 surgical nurses assessing 200 patients.</p><p><strong>Results: </strong>Post-intervention analysis indicated increased nursing confidence, with 95.7% expressing positive perception of tool use. The FLM-supported tool demonstrated a predictive accuracy of 81.3%; however, the potential for false positives or negatives remains, especially given the single-center context. Fuzzy logic stratified patients into risk groups: at risk (33.5%), borderline (20.5%), and no risk (46.0%). ANOVA analysis revealed significant differences (p < 0.05) between AKI risk and factors such as age, gender, comorbidities, clinical/laboratory parameters, surgery types, and nephrotoxic agent usage.</p><p><strong>Conclusion: </strong>While initial findings support the usability and clinical feasibility of the NURA-AKI tool, further multicenter validation is needed. The tool is designed to complement nurse judgment, promoting early AKI detection and structured risk communication in surgical care without replacing clinical autonomy.</p>","PeriodicalId":73091,"journal":{"name":"Frontiers in nephrology","volume":"5 ","pages":"1624880"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12420310/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fneph.2025.1624880","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Acute Kidney Injury (AKI) is a common yet preventable complication among surgical patients, contributing to increased morbidity, prolonged hospital stays, and higher healthcare costs. Early detection is critical; however, the absence of a standardized nursing-led risk assessment tool for AKI limits proactive intervention in clinical practice.
Objective: This study aimed to develop and evaluate the Nursing Risk Assessment for Acute Kidney Injury tool, integrating the Fuzzy Logic Model (FLM) to enhance interpretive accuracy and improve nursing-led AKI risk detection and decision-making.
Methods: A Design and Development Research (DDR) framework was employed in three phases. Phase 1 involved a needs analysis using a focus group discussion to explore the necessity of AKI assessment among surgical nurses. Phase 2 focused on tool development through expert consensus (surgeon, nephrologist, nursing academician, and experienced nurse) and evidence synthesis via a systematic literature review. In Phase 3, the Nursing Risk Assessment-AKI tool was evaluated through a quasi-experimental design at Hospital Canselor Tuanku Muhriz (HCTM), Kuala Lumpur, involving 75 surgical nurses assessing 200 patients.
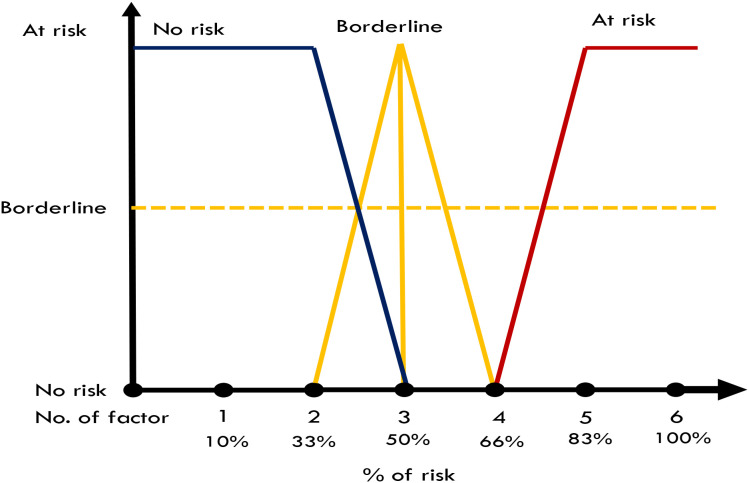
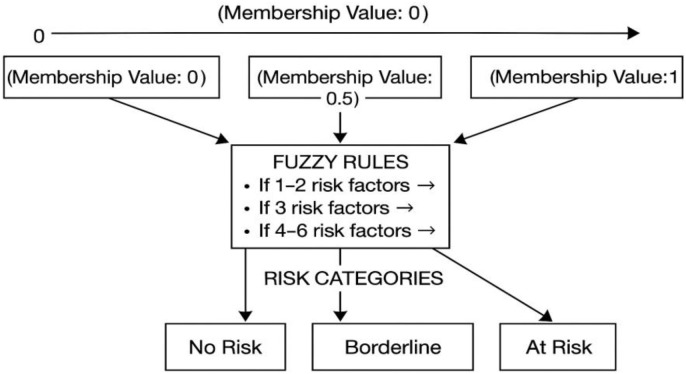
Results: Post-intervention analysis indicated increased nursing confidence, with 95.7% expressing positive perception of tool use. The FLM-supported tool demonstrated a predictive accuracy of 81.3%; however, the potential for false positives or negatives remains, especially given the single-center context. Fuzzy logic stratified patients into risk groups: at risk (33.5%), borderline (20.5%), and no risk (46.0%). ANOVA analysis revealed significant differences (p < 0.05) between AKI risk and factors such as age, gender, comorbidities, clinical/laboratory parameters, surgery types, and nephrotoxic agent usage.
Conclusion: While initial findings support the usability and clinical feasibility of the NURA-AKI tool, further multicenter validation is needed. The tool is designed to complement nurse judgment, promoting early AKI detection and structured risk communication in surgical care without replacing clinical autonomy.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


