Diagnostic value of preoperative computed tomography-urography combined with inflammatory markers in predicting lymph node metastasis in patients undergoing radical cystectomy.
Kun Yang, Mingxin Jiang, Tianyu Zhang, Yunpeng Fan, Yongde Xu, Lei Wang, Xi Zhu, Zhengguo Ji, Wei Qiu, Lang Feng, Jun Li, Daoxin Zhang, Gangyue Hao, Yinong Niu
{"title":"Diagnostic value of preoperative computed tomography-urography combined with inflammatory markers in predicting lymph node metastasis in patients undergoing radical cystectomy.","authors":"Kun Yang, Mingxin Jiang, Tianyu Zhang, Yunpeng Fan, Yongde Xu, Lei Wang, Xi Zhu, Zhengguo Ji, Wei Qiu, Lang Feng, Jun Li, Daoxin Zhang, Gangyue Hao, Yinong Niu","doi":"10.14440/bladder.2025.0012","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lymph node metastasis represents a critical prognostic factor in bladder cancer and significantly influences treatment choice and outcomes.</p><p><strong>Objective: </strong>To evaluate the predictive value of the maximum short-axis diameter of pelvic lymph nodes on preoperative computed tomography-urography (CTU), in combination with inflammatory markers, in the prediction of lymph node metastasis in radical cystectomy (RC) patients.</p><p><strong>Methods: </strong>A retrospective analysis was conducted on 210 patients who had received CTU within one month before RC at Beijing Friendship Hospital from January 2016 to December 2023. Upon screening, 174 patients were included and assigned into two groups based on postoperative pathology: i.e., lymph node metastasis group (n = 43) and non-metastasis group (n = 131). The neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and monocyte-to-lymphocyte ratio (MLR) were calculated. The maximum short-axis diameter of a lymph node ≥8 mm was considered indicative of metastasis. Receiver operating characteristic (ROC) curve analysis was performed to assess predictive performance, determine optimal cutoffs, and construct a prediction model using multivariate logistic regression.</p><p><strong>Results: </strong>Significant differences (<i>P</i> < 0.05) were observed between groups in clinical T stage, tumor grade, NLR, PLR, MLR, and CTU lymph node diameter. ROC analysis revealed optimal cutoff values for NLR (3.22), PLR (156.4), and MLR (0.62). Multivariate logistic regression identified clinical T stage, CTU lymph node diameter, MLR, and PLR as independent predictors (<i>P <</i> 0.05). The resulting model achieved an area under the curve of 0.847 (95% confidence interval: 0.777 - 0.917).</p><p><strong>Conclusion: </strong>A nomogram incorporating CTU findings, clinical T stage, MLR, and PLR effectively predicts lymph node metastasis in RC patients. However, further multi-center validation is required before clinical implementation.</p>","PeriodicalId":72421,"journal":{"name":"Bladder (San Francisco, Calif.)","volume":"12 3","pages":"e21200055"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417873/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bladder (San Francisco, Calif.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14440/bladder.2025.0012","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Lymph node metastasis represents a critical prognostic factor in bladder cancer and significantly influences treatment choice and outcomes.
Objective: To evaluate the predictive value of the maximum short-axis diameter of pelvic lymph nodes on preoperative computed tomography-urography (CTU), in combination with inflammatory markers, in the prediction of lymph node metastasis in radical cystectomy (RC) patients.
Methods: A retrospective analysis was conducted on 210 patients who had received CTU within one month before RC at Beijing Friendship Hospital from January 2016 to December 2023. Upon screening, 174 patients were included and assigned into two groups based on postoperative pathology: i.e., lymph node metastasis group (n = 43) and non-metastasis group (n = 131). The neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and monocyte-to-lymphocyte ratio (MLR) were calculated. The maximum short-axis diameter of a lymph node ≥8 mm was considered indicative of metastasis. Receiver operating characteristic (ROC) curve analysis was performed to assess predictive performance, determine optimal cutoffs, and construct a prediction model using multivariate logistic regression.
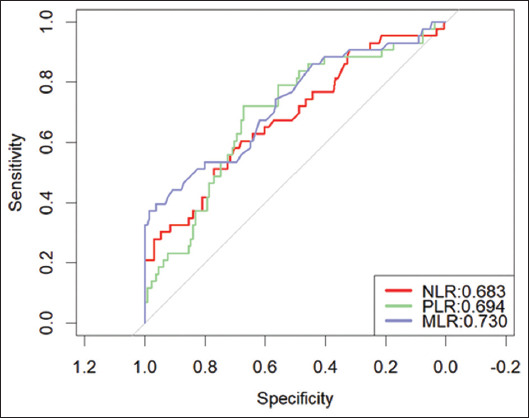
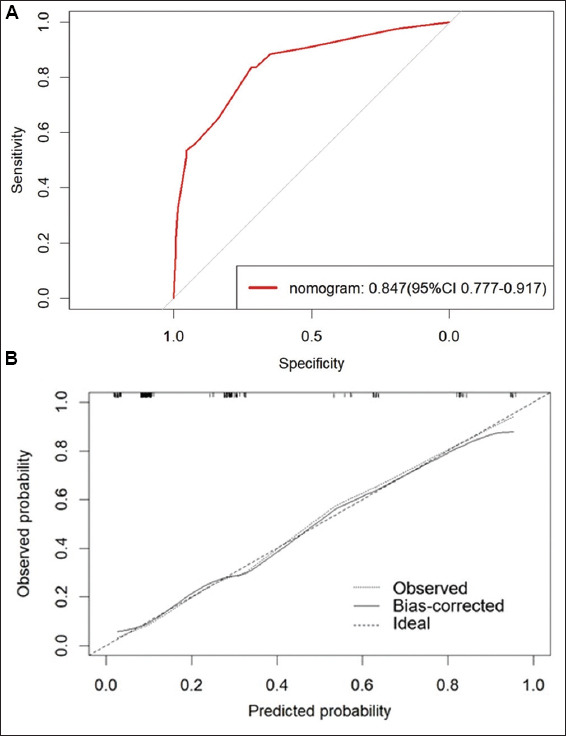
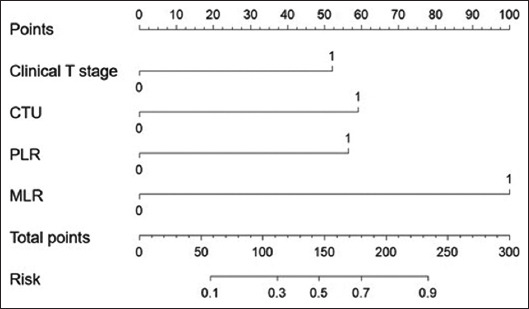
Results: Significant differences (P < 0.05) were observed between groups in clinical T stage, tumor grade, NLR, PLR, MLR, and CTU lymph node diameter. ROC analysis revealed optimal cutoff values for NLR (3.22), PLR (156.4), and MLR (0.62). Multivariate logistic regression identified clinical T stage, CTU lymph node diameter, MLR, and PLR as independent predictors (P < 0.05). The resulting model achieved an area under the curve of 0.847 (95% confidence interval: 0.777 - 0.917).
Conclusion: A nomogram incorporating CTU findings, clinical T stage, MLR, and PLR effectively predicts lymph node metastasis in RC patients. However, further multi-center validation is required before clinical implementation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


