{"title":"Extraarticular Interfragmentary Fixation of an Irreducible Pipkin Type 1 Fracture Dislocation of the Hip - A Case Report.","authors":"Dinesh Kale, Sahil Kale, Sanjay Pratheep, Ajit Modak, Ravindra Bharamgunde, Sachin Kale","doi":"10.13107/jocr.2025.v15.i09.6066","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Femoral head fractures occur almost exclusively as a result of a traumatic hip dislocation. Due to the intrinsic anatomical stability of the hip, most of these injuries result from high-energy trauma. Treatment is typically an emergency surgery that includes the reduction of the dislocated hip under anesthesia to fix the fracture of the head of the femur and reduce dislocation. Treatment outcomes tend to be inconsistent, largely because of the fracture's frequent association with pain, joint stiffness, and loss of function. Complications that are most commonly seen after femoral head fractures are osteonecrosis, osteoarthritis, and heterotopic ossification.</p><p><strong>Case report: </strong>A 39-year-old male came to casualty with an alleged history of road traffic accident with multiple fractures in bilateral upper limb, multiple rib fractures, and brachial plexus injury. Computed tomography of the pelvis with both hips was done, which showed a fracture of the left femoral head with a proximal fracture fragment found inside the acetabulum with posterior dislocation of the distal part - left femoral head fracture dislocation (Pipkin type I). Closed reduction of the hip joint failed; hence, open reduction using the Kocher-Langenbeck (KL) approach was carried out, head reduced, transfixed with guide wires, and fixed with three CC screws. On the last follow-up at the end of 1 year, the patient has regained full range of motion of the hip. Patient is able to squat, sit cross-legged, and is able to walk unaided.</p><p><strong>Conclusion: </strong>The case discussed here is one of its kind, hence fracture was also reduced after reducing the hip joint through trochanterocephalic fixation with KL approach. Precise radiographic pre-operative evaluation and early fixation with early mobilization are the key factors to success in dealing with these complex fractures. Relying on standard and textbook methods may not always yield the best outcome.</p>","PeriodicalId":16647,"journal":{"name":"Journal of Orthopaedic Case Reports","volume":"15 9","pages":"194-198"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422687/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Orthopaedic Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.13107/jocr.2025.v15.i09.6066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Femoral head fractures occur almost exclusively as a result of a traumatic hip dislocation. Due to the intrinsic anatomical stability of the hip, most of these injuries result from high-energy trauma. Treatment is typically an emergency surgery that includes the reduction of the dislocated hip under anesthesia to fix the fracture of the head of the femur and reduce dislocation. Treatment outcomes tend to be inconsistent, largely because of the fracture's frequent association with pain, joint stiffness, and loss of function. Complications that are most commonly seen after femoral head fractures are osteonecrosis, osteoarthritis, and heterotopic ossification.
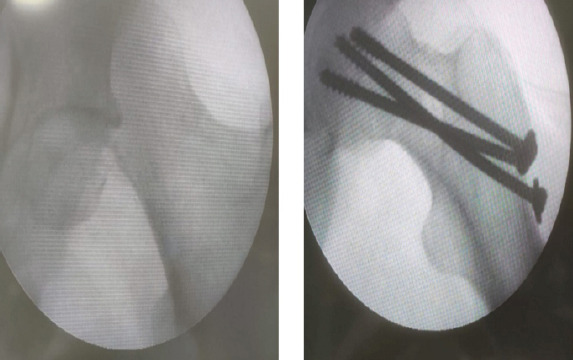
Case report: A 39-year-old male came to casualty with an alleged history of road traffic accident with multiple fractures in bilateral upper limb, multiple rib fractures, and brachial plexus injury. Computed tomography of the pelvis with both hips was done, which showed a fracture of the left femoral head with a proximal fracture fragment found inside the acetabulum with posterior dislocation of the distal part - left femoral head fracture dislocation (Pipkin type I). Closed reduction of the hip joint failed; hence, open reduction using the Kocher-Langenbeck (KL) approach was carried out, head reduced, transfixed with guide wires, and fixed with three CC screws. On the last follow-up at the end of 1 year, the patient has regained full range of motion of the hip. Patient is able to squat, sit cross-legged, and is able to walk unaided.
Conclusion: The case discussed here is one of its kind, hence fracture was also reduced after reducing the hip joint through trochanterocephalic fixation with KL approach. Precise radiographic pre-operative evaluation and early fixation with early mobilization are the key factors to success in dealing with these complex fractures. Relying on standard and textbook methods may not always yield the best outcome.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


