{"title":"A Case of Atlanto-Axial Rotatory Fixation Requiring Internal Fixation.","authors":"Ryunosuke Fukushi, Yujiro Takeshita, Tomonori Morita, Hiroki Fujita, Shunsuke Tachibana, Atsushi Teramoto","doi":"10.13107/jocr.2025.v15.i09.6082","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Most cases of atlanto-axial rotatory fixation (AARF) respond well to conservative treatment. Few reports have described initial management strategies. Almost no cases of AARF with recurrence requiring internal fixation have been reported. Here, we describe a case of recurrent AARF requiring internal fixation.</p><p><strong>Case report: </strong>A 5-year-old boy presented with a history of 22q.11.2 deletion syndrome, DiGeorge syndrome, congenital left-sided clubfoot, and periodic vomiting. He was referred to a local pediatrician with neck pain and torticollis and was prescribed analgesics. After 5 days of no improvement, he was referred to a local pediatric orthopedic hospital where he was diagnosed with AARF (Fielding classification type III). The patient was then referred to our department for traction and orthotic therapy. Computed tomography revealed no deformity of the atlanto-axial articular surface and no evidence of bony fusion between the left and right posterior arches of the atlas. Following conservative treatment, the patient's neck pain and torticollis improved, and imaging confirmed the deformity had corrected. He was discharged on day 32. The symptoms recurred on day 42, and although traction and orthotic therapies were repeated, no improvement was observed. A halo vest was applied on day 59 after symptom onset. As the deformity was corrected, the halo vest was removed on day 94 and the patient continued to wear an orthosis. The patient recurrenced on day 104 and internal fixation was performed on day 120. Two 2.4-mm hollow screws were inserted using the Magerl method. No recurrence was observed at 213 days after onset, and bone union was confirmed by imaging test, and the brace was removed.</p><p><strong>Discussion: </strong>Factors contributing to the intractability and recurrence of AARF include laxity and dysfunction of the transverse ligament. In this case, the latter was suspected because of the lax ligament structure. The patient did not undergo atlanto-axial fusion at age 5 years and vertebral bone hypoplasia was observed. Patients with a congenital element may not respond to standard conservative treatment. Thus, if the dislocation is left untreated, the lateral atlanto-axial joint may completely dislocate and drop, causing myelopathy. Thus, early internal fixation is considered desirable in such cases.</p><p><strong>Conclusion: </strong>In cases of AARF involving congenital factors, patients may not respond to standard conservative treatment. Early internal fixation should therefore be considered.</p>","PeriodicalId":16647,"journal":{"name":"Journal of Orthopaedic Case Reports","volume":"15 9","pages":"234-239"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422630/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Orthopaedic Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.13107/jocr.2025.v15.i09.6082","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Most cases of atlanto-axial rotatory fixation (AARF) respond well to conservative treatment. Few reports have described initial management strategies. Almost no cases of AARF with recurrence requiring internal fixation have been reported. Here, we describe a case of recurrent AARF requiring internal fixation.
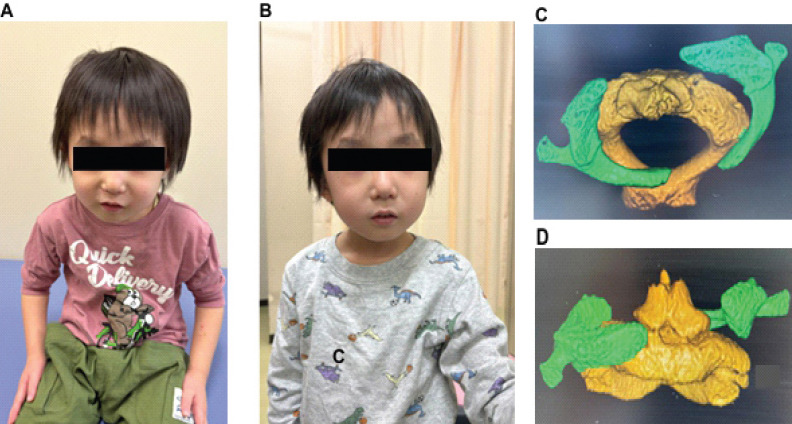
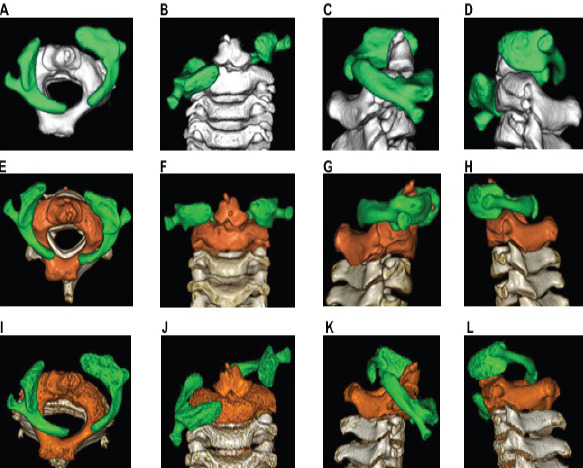
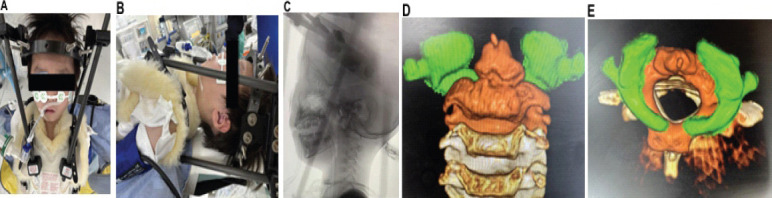
Case report: A 5-year-old boy presented with a history of 22q.11.2 deletion syndrome, DiGeorge syndrome, congenital left-sided clubfoot, and periodic vomiting. He was referred to a local pediatrician with neck pain and torticollis and was prescribed analgesics. After 5 days of no improvement, he was referred to a local pediatric orthopedic hospital where he was diagnosed with AARF (Fielding classification type III). The patient was then referred to our department for traction and orthotic therapy. Computed tomography revealed no deformity of the atlanto-axial articular surface and no evidence of bony fusion between the left and right posterior arches of the atlas. Following conservative treatment, the patient's neck pain and torticollis improved, and imaging confirmed the deformity had corrected. He was discharged on day 32. The symptoms recurred on day 42, and although traction and orthotic therapies were repeated, no improvement was observed. A halo vest was applied on day 59 after symptom onset. As the deformity was corrected, the halo vest was removed on day 94 and the patient continued to wear an orthosis. The patient recurrenced on day 104 and internal fixation was performed on day 120. Two 2.4-mm hollow screws were inserted using the Magerl method. No recurrence was observed at 213 days after onset, and bone union was confirmed by imaging test, and the brace was removed.
Discussion: Factors contributing to the intractability and recurrence of AARF include laxity and dysfunction of the transverse ligament. In this case, the latter was suspected because of the lax ligament structure. The patient did not undergo atlanto-axial fusion at age 5 years and vertebral bone hypoplasia was observed. Patients with a congenital element may not respond to standard conservative treatment. Thus, if the dislocation is left untreated, the lateral atlanto-axial joint may completely dislocate and drop, causing myelopathy. Thus, early internal fixation is considered desirable in such cases.
Conclusion: In cases of AARF involving congenital factors, patients may not respond to standard conservative treatment. Early internal fixation should therefore be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


