{"title":"Real-world management and outcomes of immune-related adverse events in German cancer care: A multicenter analysis using the SERIO registry.","authors":"Carolin Ertl, Dirk Tomsitz, Filippo Rizzo, Dirk Hempel, Lucie Heinzerling, Valeria Milani","doi":"10.1093/oncolo/oyaf275","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Immune checkpoint inhibitors (ICIs) are widely used in cancer therapy, yet diagnosing and managing immune-related adverse events (irAEs) remains challenging in clinical practice. Differences in healthcare structures between university hospitals (UH) and private practices (PP) influence irAE presentation and management, often excluding the latter from analyses.</p><p><strong>Patients and methods: </strong>This retrospective study included 604 cancer patients treated with ICIs between 2014 and 2023: 323 from UH and 281 from PP. In total, 302 irAEs were reported in the Side Effect Registry Immuno-Oncology (SERIO; http://www.serio-registry.org), with 230 cases from UH and 72 from PP. Demographics, irAE characteristics, management, and outcomes were compared between settings.</p><p><strong>Results: </strong>The UH and PP cohorts showed substantial differences. IrAEs were less frequent in the PP cohort (19% vs. 51%) and less severe (grade 3/4: 35% PP vs. 40% UH). Time to diagnosis was longer in PP (136 vs. 86 days), but treatment response rates were comparable (90% PP vs. 84% UH). UH patients experienced better symptom control (24% vs. 16%) and fewer long-term sequelae (6% vs. 10%). No irAE-related mortality occurred in either group.</p><p><strong>Conclusion: </strong>Structural differences between UH and PP impact the frequency, severity, and management of irAEs. Including underrepresented care settings in real-world analysis is essential for generating robust, generalizable evidence. By enhancing collaboration between academic institutions and community-based practitioners, we aim to improve irAE outcomes and promote more equitable, evidence-based care in immuno-oncology.</p>","PeriodicalId":54686,"journal":{"name":"Oncologist","volume":" ","pages":""},"PeriodicalIF":4.2000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12530884/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Oncologist","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/oncolo/oyaf275","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Immune checkpoint inhibitors (ICIs) are widely used in cancer therapy, yet diagnosing and managing immune-related adverse events (irAEs) remains challenging in clinical practice. Differences in healthcare structures between university hospitals (UH) and private practices (PP) influence irAE presentation and management, often excluding the latter from analyses.
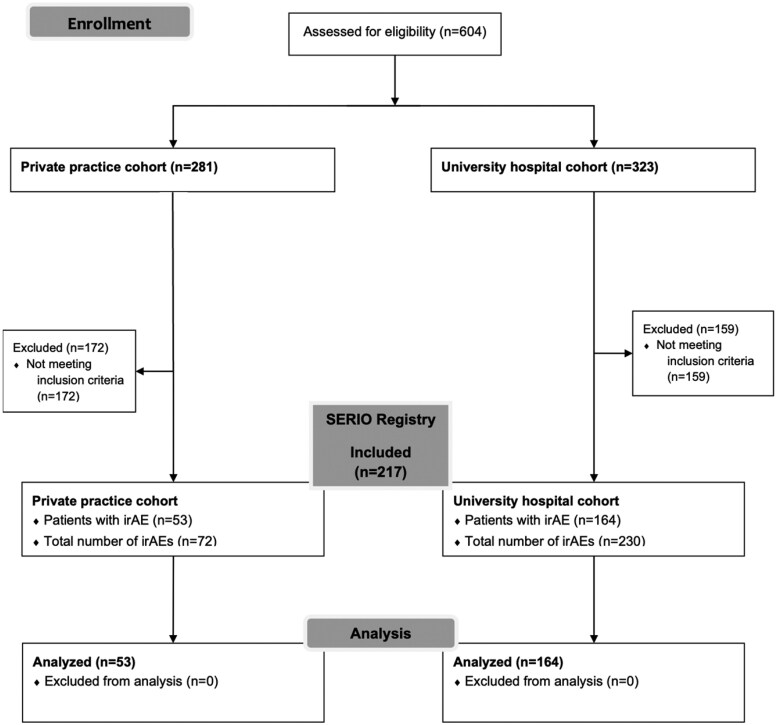
Patients and methods: This retrospective study included 604 cancer patients treated with ICIs between 2014 and 2023: 323 from UH and 281 from PP. In total, 302 irAEs were reported in the Side Effect Registry Immuno-Oncology (SERIO; http://www.serio-registry.org), with 230 cases from UH and 72 from PP. Demographics, irAE characteristics, management, and outcomes were compared between settings.
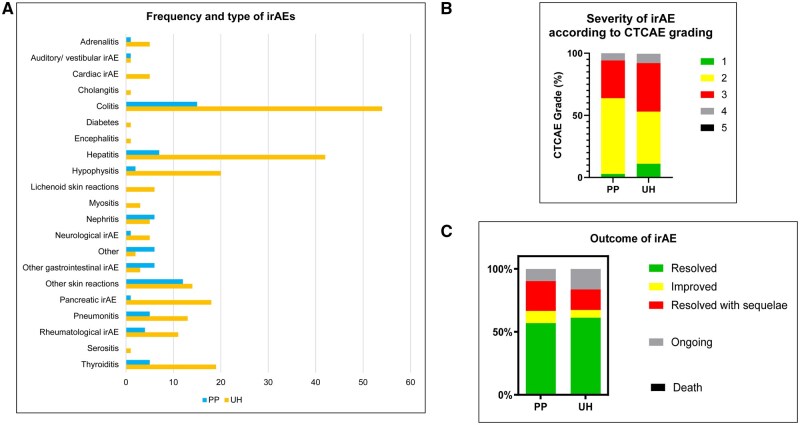
Results: The UH and PP cohorts showed substantial differences. IrAEs were less frequent in the PP cohort (19% vs. 51%) and less severe (grade 3/4: 35% PP vs. 40% UH). Time to diagnosis was longer in PP (136 vs. 86 days), but treatment response rates were comparable (90% PP vs. 84% UH). UH patients experienced better symptom control (24% vs. 16%) and fewer long-term sequelae (6% vs. 10%). No irAE-related mortality occurred in either group.
Conclusion: Structural differences between UH and PP impact the frequency, severity, and management of irAEs. Including underrepresented care settings in real-world analysis is essential for generating robust, generalizable evidence. By enhancing collaboration between academic institutions and community-based practitioners, we aim to improve irAE outcomes and promote more equitable, evidence-based care in immuno-oncology.
期刊介绍:
The Oncologist® is dedicated to translating the latest research developments into the best multidimensional care for cancer patients. Thus, The Oncologist is committed to helping physicians excel in this ever-expanding environment through the publication of timely reviews, original studies, and commentaries on important developments. We believe that the practice of oncology requires both an understanding of a range of disciplines encompassing basic science related to cancer, translational research, and clinical practice, but also the socioeconomic and psychosocial factors that determine access to care and quality of life and function following cancer treatment.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


