Bilaal Yousaf Dar, Gaayen Ravii Sahgal, Tavgah Jafar, Sangwoo R Jung, Mahmood Ahmad, Rui Bebiano Da Providencia E Costa, Iqra Javid, Syed Yousaf Ahmad, Malik Takreem Ahmad, Yusuf Abdirahman Yusuf, Abdulrahman Kashkosh
{"title":"Left ventricular unloading in patients with cardiogenic shock treated with veno-arterial extracorporeal membrane oxygenation.","authors":"Bilaal Yousaf Dar, Gaayen Ravii Sahgal, Tavgah Jafar, Sangwoo R Jung, Mahmood Ahmad, Rui Bebiano Da Providencia E Costa, Iqra Javid, Syed Yousaf Ahmad, Malik Takreem Ahmad, Yusuf Abdirahman Yusuf, Abdulrahman Kashkosh","doi":"10.1093/ehjopen/oeaf103","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Cardiogenic shock remains a significant cause of mortality despite multiple advancements in medical interventions. Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) provides crucial circulatory support but also increases left ventricular (LV) after-load, potentially worsening outcomes. Effective LV unloading strategies can enhance patient survival during VA-ECMO treatment. Our aim was to evaluate the impact of LV unloading strategies, including intra-aortic balloon pump (IABP) and Impella, on outcomes such as mortality and adverse effects in patients with cardiogenic shock treated with VA-ECMO.</p><p><strong>Methods and results: </strong>A systematic search of EMBASE and Medline was conducted from inception up to 20 August 2024. Additional sources included forward citation searches of primary references. Inclusion criteria were studies reporting mortality rates in patients undergoing VA-ECMO with and without LV unloading. Exclusion criteria included case studies, editorials, commentaries, literature reviews, studies without a control group, those not examining LV unloading, studies on non-cardiogenic shock patients, and paediatric populations. From 943 identified studies, 26 met the inclusion criteria after abstract and full text screening by two authors. Data extraction followed PRISMA guidelines with independent reviewers abstracting data and assessing study quality using the Cochrane Risk of Bias in non-randomized studies (ROBINS-I) tool. A random-effects model was used to pool data, accounting for study heterogeneity. The primary outcome was all-cause mortality, assessed at three time points: intra-hospital mortality, 30-day mortality and mortality at longest available follow-up. Secondary outcomes included adverse effects such as bleeding, infection, cardiovascular events, limb ischaemia, and renal replacement therapy (RRT). The meta-analysis included 26 studies with a total of 22 625 patients. LV unloading strategies significantly reduced mortality compared to no unloading (RR: 0.80; 95% CI: 0.73 to 0.96). IABP (RR: 0.78; 95% CI: 0.69 to 0.89) was associated with a significant reduction of mortality compared to no unloading. All adverse effects were comparable across groups apart from significantly increased infection rates and need for RRT in Impella patients (RR: 1.37; 95% CI: 1.07 to 1.75, and RR: 2.02; 95% CI: 1.37 to 3.00, respectively).</p><p><strong>Conclusion: </strong>LV unloading strategies associated with reduced mortality in patients with cardiogenic shock treated with VA-ECMO. Whilst adverse effects are similar across all strategies, Impella specifically is linked to higher infection rates and need for RRT. These findings could be used to support the use of LV unloading devices in clinical practice and highlight the need for further randomized controlled trials to establish optimal device-options and management protocols.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 5","pages":"oeaf103"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415181/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf103","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
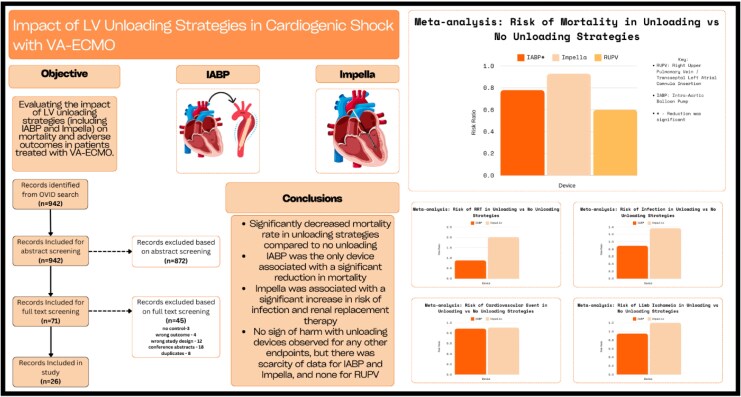
Aims: Cardiogenic shock remains a significant cause of mortality despite multiple advancements in medical interventions. Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) provides crucial circulatory support but also increases left ventricular (LV) after-load, potentially worsening outcomes. Effective LV unloading strategies can enhance patient survival during VA-ECMO treatment. Our aim was to evaluate the impact of LV unloading strategies, including intra-aortic balloon pump (IABP) and Impella, on outcomes such as mortality and adverse effects in patients with cardiogenic shock treated with VA-ECMO.
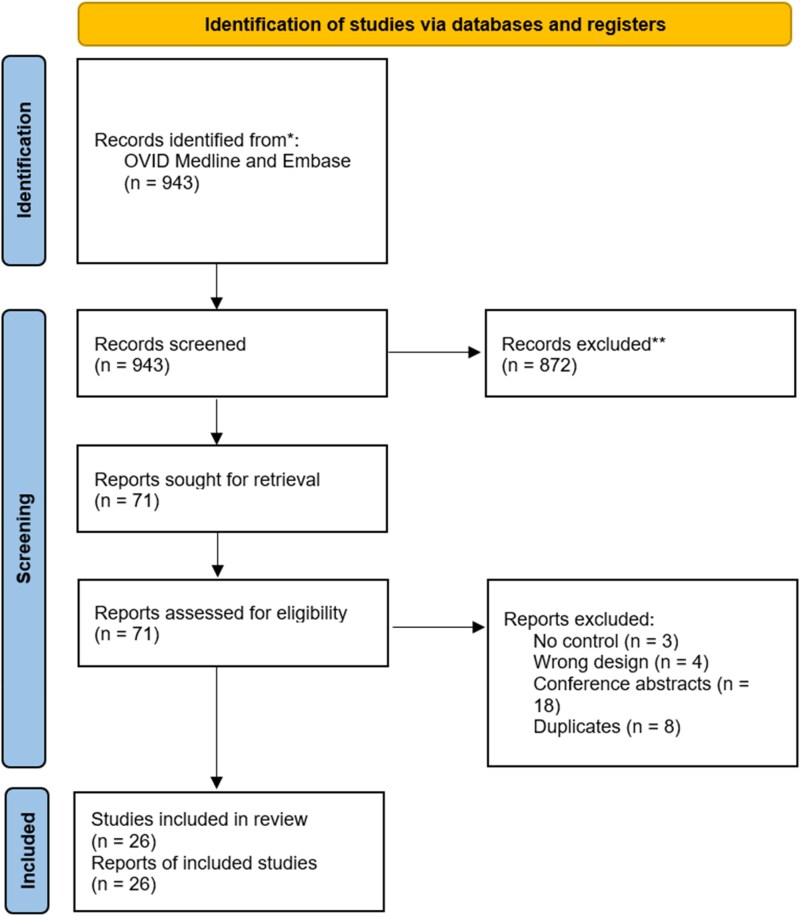
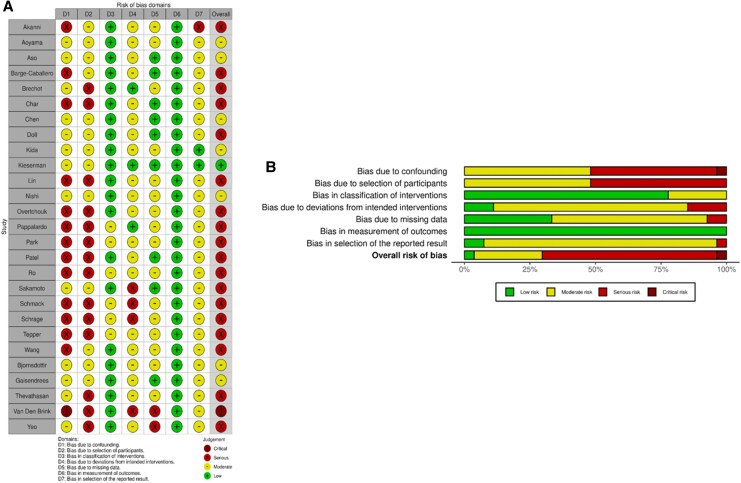
Methods and results: A systematic search of EMBASE and Medline was conducted from inception up to 20 August 2024. Additional sources included forward citation searches of primary references. Inclusion criteria were studies reporting mortality rates in patients undergoing VA-ECMO with and without LV unloading. Exclusion criteria included case studies, editorials, commentaries, literature reviews, studies without a control group, those not examining LV unloading, studies on non-cardiogenic shock patients, and paediatric populations. From 943 identified studies, 26 met the inclusion criteria after abstract and full text screening by two authors. Data extraction followed PRISMA guidelines with independent reviewers abstracting data and assessing study quality using the Cochrane Risk of Bias in non-randomized studies (ROBINS-I) tool. A random-effects model was used to pool data, accounting for study heterogeneity. The primary outcome was all-cause mortality, assessed at three time points: intra-hospital mortality, 30-day mortality and mortality at longest available follow-up. Secondary outcomes included adverse effects such as bleeding, infection, cardiovascular events, limb ischaemia, and renal replacement therapy (RRT). The meta-analysis included 26 studies with a total of 22 625 patients. LV unloading strategies significantly reduced mortality compared to no unloading (RR: 0.80; 95% CI: 0.73 to 0.96). IABP (RR: 0.78; 95% CI: 0.69 to 0.89) was associated with a significant reduction of mortality compared to no unloading. All adverse effects were comparable across groups apart from significantly increased infection rates and need for RRT in Impella patients (RR: 1.37; 95% CI: 1.07 to 1.75, and RR: 2.02; 95% CI: 1.37 to 3.00, respectively).
Conclusion: LV unloading strategies associated with reduced mortality in patients with cardiogenic shock treated with VA-ECMO. Whilst adverse effects are similar across all strategies, Impella specifically is linked to higher infection rates and need for RRT. These findings could be used to support the use of LV unloading devices in clinical practice and highlight the need for further randomized controlled trials to establish optimal device-options and management protocols.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


