Markella I Printezi, Arco J Teske, Nicolaas P A Zuithoff, Kim Urgel, Rhodé M Bijlsma, Anna van Rhenen, Maarten Jan Cramer, Cornelis J A Punt, Anne M May, Linda W van Laake
{"title":"Morning administration of anthracyclines is associated with a lower risk of cancer therapy-related cardiac dysfunction.","authors":"Markella I Printezi, Arco J Teske, Nicolaas P A Zuithoff, Kim Urgel, Rhodé M Bijlsma, Anna van Rhenen, Maarten Jan Cramer, Cornelis J A Punt, Anne M May, Linda W van Laake","doi":"10.1093/ehjopen/oeaf100","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Pre-clinical studies point towards an administration time-dependency of anthracycline-induced cancer therapy-related cardiac dysfunction (CTRCD). This retrospective study aimed to investigate the association between time-of-day of AC administration and CTRCD.</p><p><strong>Methods and results: </strong>Patients from two cardio-oncology outpatient clinics, treated with ACs for any malignancy, were included. Percentage of afternoon AC administration was calculated: cumulative dose administered in the afternoon (12 p.m.-11:59 p.m.)/total cumulative dose. Three groups were defined: morning group ≥ 50% of ACs in the morning (12 a.m.-11:59 a.m.), afternoon group ≥ 50% of ACs in the afternoon, and intermediate group = exactly 50% of ACs in the morning and afternoon. Associations between AC timing and occurrence of CTRCD and heart failure (HF) were assessed using survival analyses. Of 270 included patients, 66 developed CTRCD and 17 developed HF. Compared with the morning group, the afternoon group had a higher risk of developing CTRCD: hazard ratio (HR) 2.88 (95% CI: 1.52-5.44). When considering percentage of ACs administered in the afternoon as a continuous variable, the HR for developing CTRCD was 1.14 (95% CI: 1.04-1.24) for each subsequent 10% of afternoon administration. Results were consistent across sensitivity analyses of age, sex, body mass index, malignancy type, cumulative AC dose, and HFA-ICOS risk score. Congruently, the continuous variable of afternoon AC administration was associated with higher risk of HF: HR = 1.19 (95% CI: 1.01-1.41).</p><p><strong>Conclusion: </strong>Afternoon administration of ACs is associated with an increased risk of developing CTRCD and HF, suggesting that morning administration may be preferred. Before widespread implementation, these findings should be confirmed in an RCT.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 5","pages":"oeaf100"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415182/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf100","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
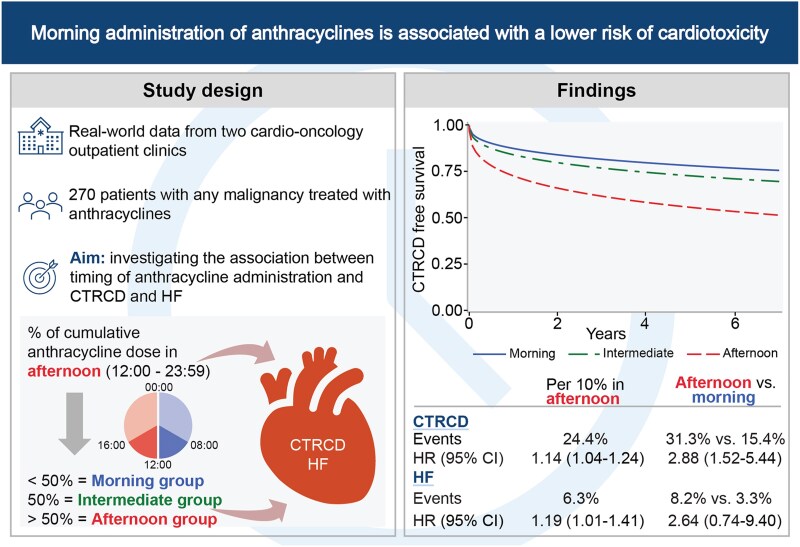
Aims: Pre-clinical studies point towards an administration time-dependency of anthracycline-induced cancer therapy-related cardiac dysfunction (CTRCD). This retrospective study aimed to investigate the association between time-of-day of AC administration and CTRCD.
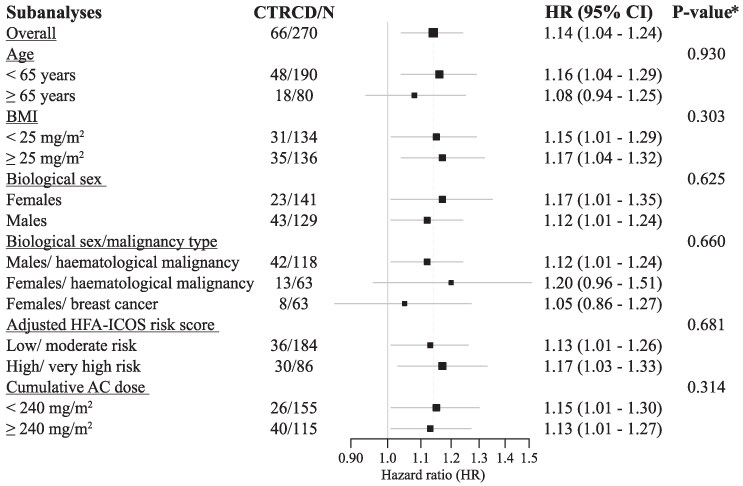
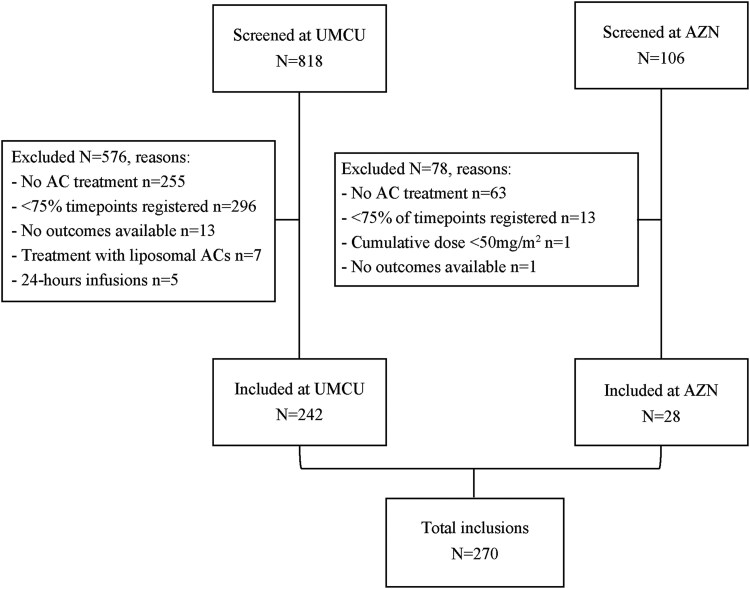
Methods and results: Patients from two cardio-oncology outpatient clinics, treated with ACs for any malignancy, were included. Percentage of afternoon AC administration was calculated: cumulative dose administered in the afternoon (12 p.m.-11:59 p.m.)/total cumulative dose. Three groups were defined: morning group ≥ 50% of ACs in the morning (12 a.m.-11:59 a.m.), afternoon group ≥ 50% of ACs in the afternoon, and intermediate group = exactly 50% of ACs in the morning and afternoon. Associations between AC timing and occurrence of CTRCD and heart failure (HF) were assessed using survival analyses. Of 270 included patients, 66 developed CTRCD and 17 developed HF. Compared with the morning group, the afternoon group had a higher risk of developing CTRCD: hazard ratio (HR) 2.88 (95% CI: 1.52-5.44). When considering percentage of ACs administered in the afternoon as a continuous variable, the HR for developing CTRCD was 1.14 (95% CI: 1.04-1.24) for each subsequent 10% of afternoon administration. Results were consistent across sensitivity analyses of age, sex, body mass index, malignancy type, cumulative AC dose, and HFA-ICOS risk score. Congruently, the continuous variable of afternoon AC administration was associated with higher risk of HF: HR = 1.19 (95% CI: 1.01-1.41).
Conclusion: Afternoon administration of ACs is associated with an increased risk of developing CTRCD and HF, suggesting that morning administration may be preferred. Before widespread implementation, these findings should be confirmed in an RCT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


