Monocyte Anisocytosis Can Discriminate Between Sepsis and Sterile Inflammation, but not Mortality, in Critically Ill Surgical/Trauma Patients: A Secondary Prospective Analysis.
Miguel Hernández-Ríos, Ruoxuan Wu, Valerie A Polcz, Rachel D Burnside, Lael M Yonker, Daniel Irimia, Feifei Xiao, Jaimar C Rincon, Tyler J Loftus, Lyle L Moldawer, Robert Maile, Philip A Efron, Muxuan Liang
{"title":"Monocyte Anisocytosis Can Discriminate Between Sepsis and Sterile Inflammation, but not Mortality, in Critically Ill Surgical/Trauma Patients: A Secondary Prospective Analysis.","authors":"Miguel Hernández-Ríos, Ruoxuan Wu, Valerie A Polcz, Rachel D Burnside, Lael M Yonker, Daniel Irimia, Feifei Xiao, Jaimar C Rincon, Tyler J Loftus, Lyle L Moldawer, Robert Maile, Philip A Efron, Muxuan Liang","doi":"10.1097/CCE.0000000000001309","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives background: </strong>Monocyte anisocytosis (monocyte distribution width [MDW]) has been previously validated to predict sepsis and outcome in patients presenting in the emergency department and mixed-population ICUs. Determining sepsis in a critically ill surgical/trauma population is often difficult due to concomitant inflammation and stress. We examined whether MDW could identify sepsis among patients admitted to a surgical/trauma ICU and predict clinical outcome.</p><p><strong>Design: </strong>Secondary analysis of three prospective observational clinical studies.</p><p><strong>Setting: </strong>Single institution ICU.</p><p><strong>Patients/subjects: </strong>Two hundred thirty-eight participants were included in this study: 107 patients who were admitted to the ICU and adjudicated to have sepsis, 80 patients who were considered critically ill nonseptic (CINS), and 51 healthy control participants.</p><p><strong>Interventions: </strong>MDW was measured among hospitalized patients admitted to the ICU with the diagnosis of sepsis or CINS patients at risk of developing sepsis. Blood samples were collected at admission and at intervals during ICU admission.</p><p><strong>Measurements and main results: </strong>MDW significantly differed between septic and CINS patients on ICU admission (26.4, interquartile range [IQR, 23.5-30.8] vs. 20.1 [IQR, 17.9-21.9]; p < 0.001) and could discriminate with an area under the receiver operating characteristic curve of 0.85 (95% CI, 0.79-0.91; p < 0.001). An MDW of greater than 22.0 at admission to the ICU could identify sepsis with a 78% specificity and a 90% sensitivity but could not discriminate in-hospital, 30-day, or 90-day mortality.</p><p><strong>Limitations: </strong>Small sample size from a single institution. Our analysis did not include other relevant biomarkers such as procalcitonin, C-reactive protein, and interleukin-6. In the imputation of missing values, linear mixed-effect models were used, risking model misspecification and the violation of the missing-at-random assumption.</p><p><strong>Conclusions: </strong>Among surgical/trauma ICU patients, MDW can discriminate between sepsis and nonseptic inflammation, but it is a weak predictor of mortality.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 9","pages":"e1309"},"PeriodicalIF":2.7000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422779/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001309","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives background: Monocyte anisocytosis (monocyte distribution width [MDW]) has been previously validated to predict sepsis and outcome in patients presenting in the emergency department and mixed-population ICUs. Determining sepsis in a critically ill surgical/trauma population is often difficult due to concomitant inflammation and stress. We examined whether MDW could identify sepsis among patients admitted to a surgical/trauma ICU and predict clinical outcome.
Design: Secondary analysis of three prospective observational clinical studies.
Setting: Single institution ICU.
Patients/subjects: Two hundred thirty-eight participants were included in this study: 107 patients who were admitted to the ICU and adjudicated to have sepsis, 80 patients who were considered critically ill nonseptic (CINS), and 51 healthy control participants.
Interventions: MDW was measured among hospitalized patients admitted to the ICU with the diagnosis of sepsis or CINS patients at risk of developing sepsis. Blood samples were collected at admission and at intervals during ICU admission.
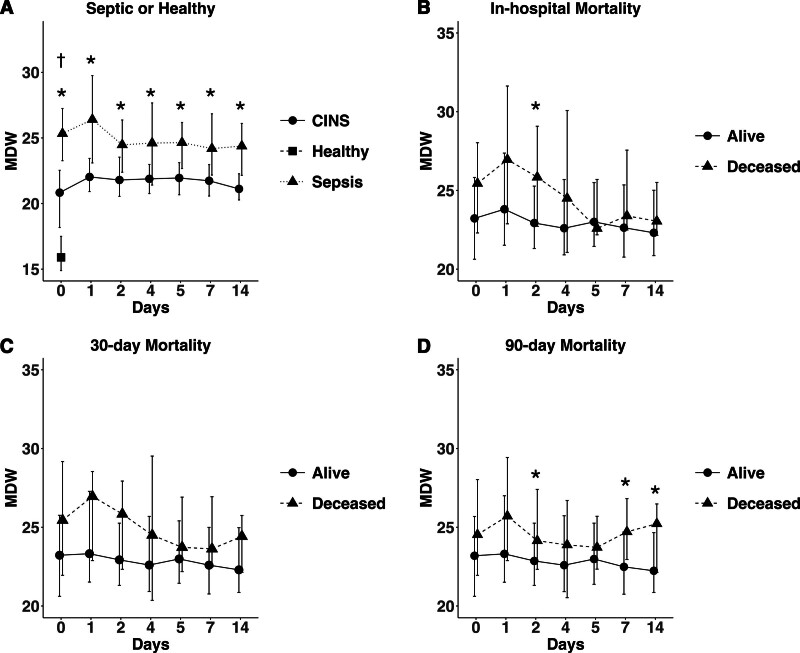
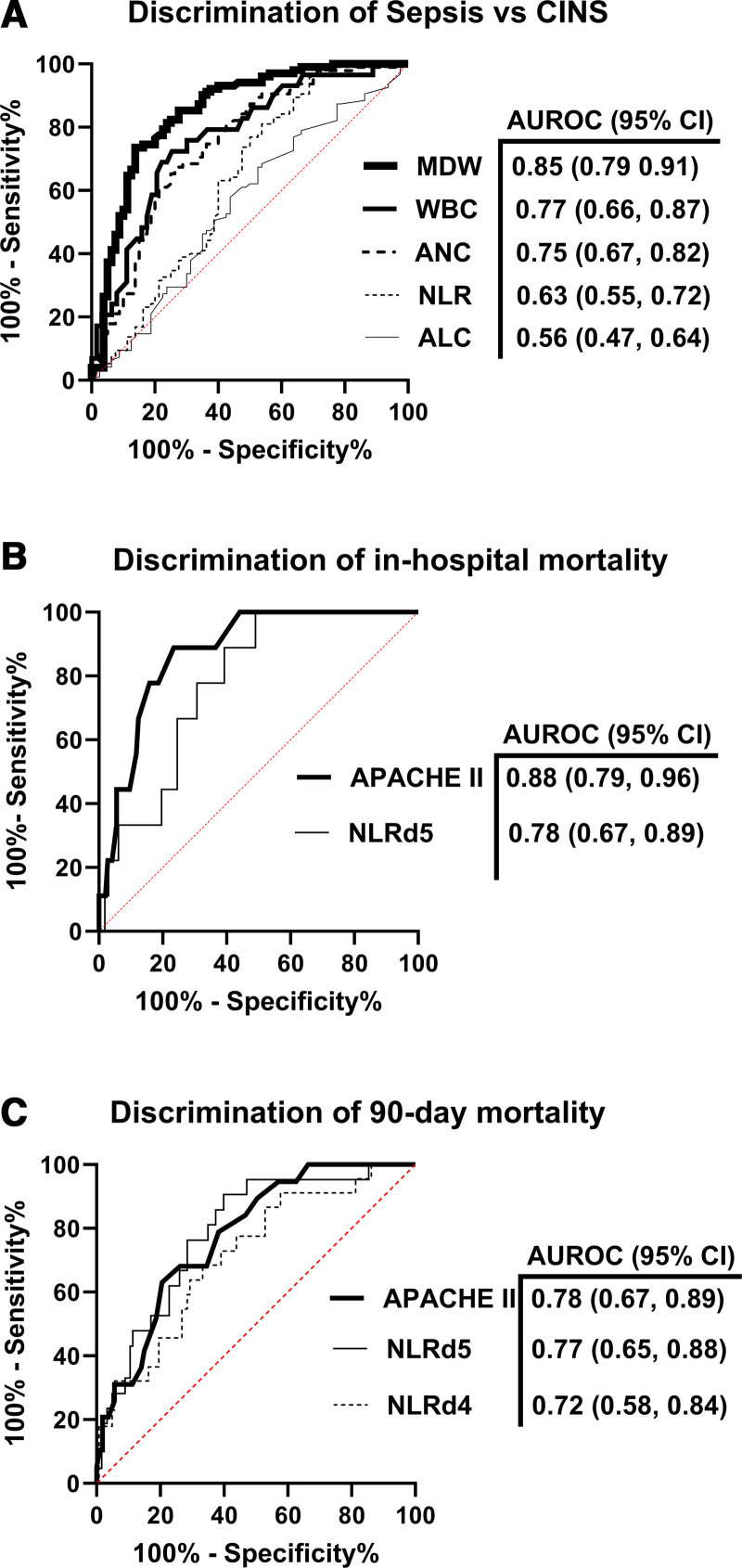
Measurements and main results: MDW significantly differed between septic and CINS patients on ICU admission (26.4, interquartile range [IQR, 23.5-30.8] vs. 20.1 [IQR, 17.9-21.9]; p < 0.001) and could discriminate with an area under the receiver operating characteristic curve of 0.85 (95% CI, 0.79-0.91; p < 0.001). An MDW of greater than 22.0 at admission to the ICU could identify sepsis with a 78% specificity and a 90% sensitivity but could not discriminate in-hospital, 30-day, or 90-day mortality.
Limitations: Small sample size from a single institution. Our analysis did not include other relevant biomarkers such as procalcitonin, C-reactive protein, and interleukin-6. In the imputation of missing values, linear mixed-effect models were used, risking model misspecification and the violation of the missing-at-random assumption.
Conclusions: Among surgical/trauma ICU patients, MDW can discriminate between sepsis and nonseptic inflammation, but it is a weak predictor of mortality.
目的背景:单核细胞异数(单核细胞分布宽度[MDW])先前已被证实可以预测急诊科和混合人群icu患者的脓毒症和预后。由于伴随的炎症和应激,在危重外科/创伤人群中确定败血症通常是困难的。我们研究了MDW是否可以在外科/创伤ICU收治的患者中识别败血症并预测临床结果。设计:对三项前瞻性观察性临床研究进行二次分析。环境:单机构ICU。患者/受试者:本研究纳入了238名参与者:107名被诊断为脓毒症的ICU患者,80名被认为是重症非脓毒症(CINS)的患者,以及51名健康对照参与者。干预措施:在诊断为败血症的ICU住院患者或有发生败血症风险的CINS患者中测量MDW。在入院时和ICU住院期间每隔一段时间采集一次血样。测量结果及主要结果:脓毒症患者与CINS患者在ICU入院时的MDW差异显著(26.4,四分位数范围[IQR, 23.5-30.8] vs. 20.1 [IQR, 17.9-21.9], p < 0.001),可与受试者工作特征曲线下面积0.85区分(95% CI, 0.79-0.91, p < 0.001)。ICU入院时MDW大于22.0可以以78%的特异性和90%的敏感性识别脓毒症,但不能区分住院、30天或90天死亡率。局限性:来自单一机构的样本量小。我们的分析没有包括其他相关的生物标志物,如降钙素原、c反应蛋白和白细胞介素-6。在缺失值的imputation中,使用了线性混合效应模型,这有可能导致模型规格错误和违反missing-at-random假设。结论:在外科/创伤ICU患者中,MDW可以区分脓毒症和非脓毒症炎症,但它是死亡率的弱预测因子。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


