James Allen, Samir Asmar, James Vun, Adrian Andronic, Luke Budworth, Paul David Cowling, Mr Mantaran Bakshi, Dr Nikhil Bhuskute, Mr David Bowe, Mr Simon Boyle, Dr Christian Chew, Mr Ahmed Elattar, Ms Madeline Fale, Dr Neesha Jenkins, Mr Paul McCormack, Dr Pankaj Nagtode, Mr Neil Pennington, Mr James Tyler, Mr Mathew Varghese, Mr Phil Wright
{"title":"Predictors of reintervention following hydrodistension as a treatment for adhesive capsulitis : a multicentre retrospective study.","authors":"James Allen, Samir Asmar, James Vun, Adrian Andronic, Luke Budworth, Paul David Cowling, Mr Mantaran Bakshi, Dr Nikhil Bhuskute, Mr David Bowe, Mr Simon Boyle, Dr Christian Chew, Mr Ahmed Elattar, Ms Madeline Fale, Dr Neesha Jenkins, Mr Paul McCormack, Dr Pankaj Nagtode, Mr Neil Pennington, Mr James Tyler, Mr Mathew Varghese, Mr Phil Wright","doi":"10.1302/2633-1462.69.BJO-2025-0001.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The primary outcome was to determine the proportion of patients with adhesive capsulitis who required reintervention following a treatment of hydrodistension. The secondary outcome was to identify predictors of reintervention.</p><p><strong>Methods: </strong>A total of 712 hydrodistension procedures from six NHS trusts were included for statistical analysis. Minimum follow-up was 18 months. The primary outcome was the reintervention rate. Reintervention was defined as a subsequent steroid injection, arthroscopic capsular release, or repeat hydrodistension. The secondary outcome was to determine predictors of reintervention. Patient demographic characteristics, duration of symptoms, previous treatment, diabetic status, insulin usage, and glycated haemoglobin (HbA1c) were recorded. Logistic regression models were run for the primary and secondary outcomes.</p><p><strong>Results: </strong>In total, 176/712 patients (24.7%) required further treatment. We found the following factors to be predictors of repeat intervention: female sex (p = 0.036), diabetics (p = 0.003), patients with a HbA1c ≥ 48 mmol/mol (p = 0.011), and patients who had received previous steroid injections (p = 0.002). Age and duration of symptoms did not correlate with increased risk of reintervention.</p><p><strong>Conclusion: </strong>Hydrodistension may be considered an effective treatment for adhesive capsulitis, with the majority of patients in our cohort not requiring further intervention. We identified predictors of reintervention, which may assist in patient counselling and treatment planning. Although the optimal first-line management for adhesive capsulitis remains uncertain, hydrodistension represents a cost-effective, widely accessible, and minimally invasive option. Further comparative studies are warranted to establish its place in the treatment algorithm.</p>","PeriodicalId":34103,"journal":{"name":"Bone & Joint Open","volume":"6 9","pages":"1073-1079"},"PeriodicalIF":3.1000,"publicationDate":"2025-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417055/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1302/2633-1462.69.BJO-2025-0001.R1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: The primary outcome was to determine the proportion of patients with adhesive capsulitis who required reintervention following a treatment of hydrodistension. The secondary outcome was to identify predictors of reintervention.
Methods: A total of 712 hydrodistension procedures from six NHS trusts were included for statistical analysis. Minimum follow-up was 18 months. The primary outcome was the reintervention rate. Reintervention was defined as a subsequent steroid injection, arthroscopic capsular release, or repeat hydrodistension. The secondary outcome was to determine predictors of reintervention. Patient demographic characteristics, duration of symptoms, previous treatment, diabetic status, insulin usage, and glycated haemoglobin (HbA1c) were recorded. Logistic regression models were run for the primary and secondary outcomes.
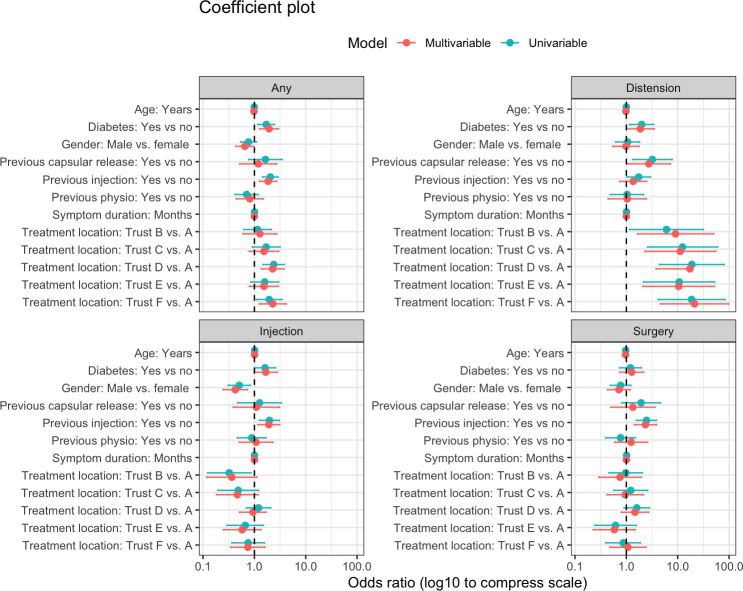
Results: In total, 176/712 patients (24.7%) required further treatment. We found the following factors to be predictors of repeat intervention: female sex (p = 0.036), diabetics (p = 0.003), patients with a HbA1c ≥ 48 mmol/mol (p = 0.011), and patients who had received previous steroid injections (p = 0.002). Age and duration of symptoms did not correlate with increased risk of reintervention.
Conclusion: Hydrodistension may be considered an effective treatment for adhesive capsulitis, with the majority of patients in our cohort not requiring further intervention. We identified predictors of reintervention, which may assist in patient counselling and treatment planning. Although the optimal first-line management for adhesive capsulitis remains uncertain, hydrodistension represents a cost-effective, widely accessible, and minimally invasive option. Further comparative studies are warranted to establish its place in the treatment algorithm.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


