Gabriela Zavala Wong, Maclean S Panshin, Tina Samsamshariat, Mohamed Albirair, Jakob E Gamboa, Colby G Simmons, Ashley D Farley, Lacey N LaGrone
{"title":"Dissecting inequity: global systematic review of trauma clinical guidance.","authors":"Gabriela Zavala Wong, Maclean S Panshin, Tina Samsamshariat, Mohamed Albirair, Jakob E Gamboa, Colby G Simmons, Ashley D Farley, Lacey N LaGrone","doi":"10.1136/tsaco-2024-001624","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Efforts to strengthen healthcare systems have led to the development of clinical practice guidance, defined as clinical decision-making aids built on scientific evidence, experiential knowledge, and ideally, patient values. This review evaluates the accessibility, relevance, and quality of existing trauma guidance globally.</p><p><strong>Methods: </strong>A systematic review evaluated trauma-related clinical guidance sources published from 2016 to 2023, searching in English across eight databases and 28 professional society websites. Using a combination of Medical Subject Headings terms, a series of protocols, guidelines, position articles, reviews and consensus documents were assessed using the National Guideline Clearinghouse Extent Adherence to Trustworthy Standards (NEATS).</p><p><strong>Results: </strong>Out of 986 records, 108 met review criteria, excluding unretrievable (13), outdated (25), non-trauma (110), and not fitting a guidance resource definition (730). Almost 90% of trauma guidance resources featured a first author from a high-income country (HIC). When categorizing trauma guidance resources by the first author's region, 44% came from North America, 8% from South America, 34% from Europe, 13% from Asia and Pacific and 1% from Africa. 82% of clinical guidance was public access with no registration required, and the remaining 18% had an average cost of US$45.7 (13.38 SD) the majority of which was generated by US trauma professional organizations. Regarding quality standard adherence, the mean quality score of all sources was 3.81 (scale 1-5), 77% disclosed the source of funding, 91% involved a multidisciplinary group and 54% explicitly mentioned the inclusion of a methodological expert. On logistic regression, the only factor predictive of a high (≥4) NEATS quality score was the presence of a methodological expert. There was no observed association between quality and language, author origin, multidisciplinary group, and professional society endorsement.</p><p><strong>Discussion: </strong>Retrieved articles were mostly published in English and predominantly produced by HIC authors. Low- and middle-income country (LMIC) researchers relied on collaboration for most publications. Most resources were open access, however, the average cost for those which require paid access (US$45.7) may be cost-prohibitive to LMIC providers. Generally, clinical practice guidance resources have a fair quality score when evaluated with the NEATS scorecard. Nonetheless, methodological expert involvement is often overlooked, despite its impact on guidance resources quality. Limitations of this review include the exclusive use of English for search terms, which may have led to the under-representation of sources in other languages and those from LMIC regions.</p><p><strong>Conclusion: </strong>The reviewed trauma clinical guidance published between 2016 and 2023 predominantly featured authors from HICs, with limited representation from LMICs, despite LMICs bearing a higher injury burden. Only 14% of guidance considered pediatric populations, although trauma is the leading cause of death among this group. Most guidance was published in English, with over 80% being open access. The mean quality score of included guidance, assessed by the NEATS scorecard, was 3.81 out of 5. Enhancing trauma guidance impact may require promoting LMIC authorship, fostering multiregional collaborations and addressing barriers such as cost, registration and language.</p>","PeriodicalId":23307,"journal":{"name":"Trauma Surgery & Acute Care Open","volume":"10 Suppl 5","pages":"e001624"},"PeriodicalIF":2.2000,"publicationDate":"2025-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414201/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Trauma Surgery & Acute Care Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/tsaco-2024-001624","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Efforts to strengthen healthcare systems have led to the development of clinical practice guidance, defined as clinical decision-making aids built on scientific evidence, experiential knowledge, and ideally, patient values. This review evaluates the accessibility, relevance, and quality of existing trauma guidance globally.
Methods: A systematic review evaluated trauma-related clinical guidance sources published from 2016 to 2023, searching in English across eight databases and 28 professional society websites. Using a combination of Medical Subject Headings terms, a series of protocols, guidelines, position articles, reviews and consensus documents were assessed using the National Guideline Clearinghouse Extent Adherence to Trustworthy Standards (NEATS).
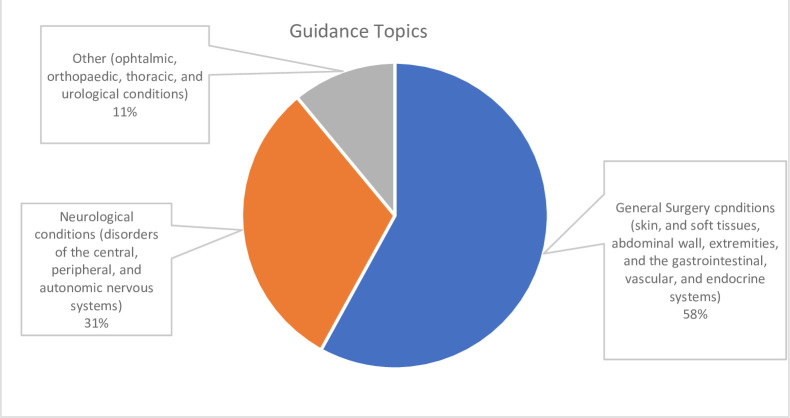
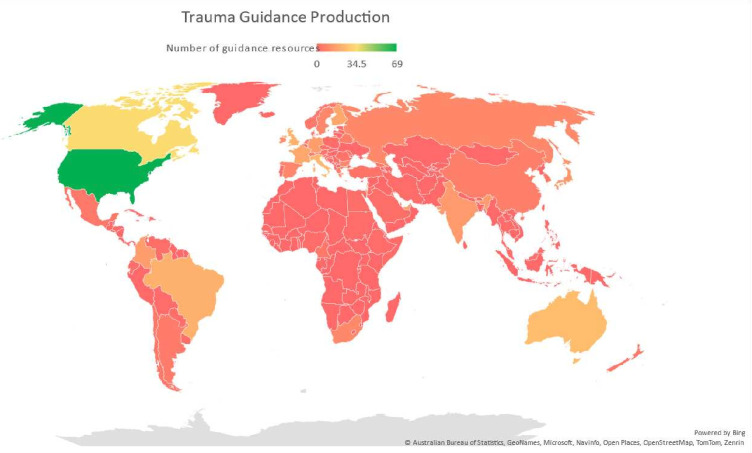
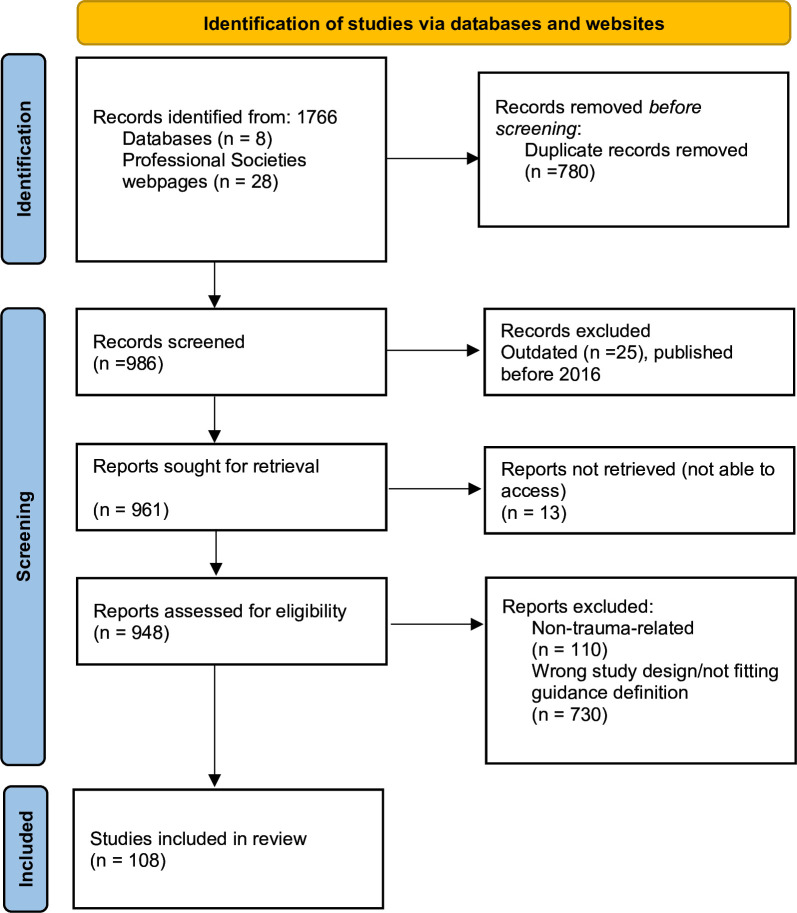
Results: Out of 986 records, 108 met review criteria, excluding unretrievable (13), outdated (25), non-trauma (110), and not fitting a guidance resource definition (730). Almost 90% of trauma guidance resources featured a first author from a high-income country (HIC). When categorizing trauma guidance resources by the first author's region, 44% came from North America, 8% from South America, 34% from Europe, 13% from Asia and Pacific and 1% from Africa. 82% of clinical guidance was public access with no registration required, and the remaining 18% had an average cost of US$45.7 (13.38 SD) the majority of which was generated by US trauma professional organizations. Regarding quality standard adherence, the mean quality score of all sources was 3.81 (scale 1-5), 77% disclosed the source of funding, 91% involved a multidisciplinary group and 54% explicitly mentioned the inclusion of a methodological expert. On logistic regression, the only factor predictive of a high (≥4) NEATS quality score was the presence of a methodological expert. There was no observed association between quality and language, author origin, multidisciplinary group, and professional society endorsement.
Discussion: Retrieved articles were mostly published in English and predominantly produced by HIC authors. Low- and middle-income country (LMIC) researchers relied on collaboration for most publications. Most resources were open access, however, the average cost for those which require paid access (US$45.7) may be cost-prohibitive to LMIC providers. Generally, clinical practice guidance resources have a fair quality score when evaluated with the NEATS scorecard. Nonetheless, methodological expert involvement is often overlooked, despite its impact on guidance resources quality. Limitations of this review include the exclusive use of English for search terms, which may have led to the under-representation of sources in other languages and those from LMIC regions.
Conclusion: The reviewed trauma clinical guidance published between 2016 and 2023 predominantly featured authors from HICs, with limited representation from LMICs, despite LMICs bearing a higher injury burden. Only 14% of guidance considered pediatric populations, although trauma is the leading cause of death among this group. Most guidance was published in English, with over 80% being open access. The mean quality score of included guidance, assessed by the NEATS scorecard, was 3.81 out of 5. Enhancing trauma guidance impact may require promoting LMIC authorship, fostering multiregional collaborations and addressing barriers such as cost, registration and language.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


