Maria Chara Stylianidi, Sascha Vaghiri, Peter C Ambe, Wolfram Trudo Knoefel, Dimitrios Prassas
{"title":"The role of remote ischaemic preconditioning (RIPC) in colorectal surgery: a meta-analysis of randomized-controlled studies.","authors":"Maria Chara Stylianidi, Sascha Vaghiri, Peter C Ambe, Wolfram Trudo Knoefel, Dimitrios Prassas","doi":"10.1007/s00423-025-03864-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Remote ischaemic preconditioning (RIPC) which consists of repeated brief episodes of non-lethal limb ischaemia is associated with organ protection and improved clinical outcomes through complex pathophysiological pathways. The aim of this meta-analysis was to evaluate the postoperative effects of RIPC in bowel recovery and surgical morbidity after colorectal surgery.</p><p><strong>Methods: </strong>In strict adherence to the PRISMA guidelines, a systematic literature search was performed for studies comparing the postoperative effect RIPC in colorectal surgery. Data from eligible studies were extracted, qualitatively assessed, and included. Odds ratios (OR) and standardized mean differences (SMDs) with 95% confidence intervals (CIs) were calculated.</p><p><strong>Results: </strong>Four studies with a total of 311 patients were included. RIPC resulted in reduced rates of postoperative ileus (POI) (OR 0.42, 95% CI 0.21-0.85, p = 0.02) and lower postoperative TNF-α levels (SMD - 1.01, 95% CI -1.59,-0.43, p = 0.0007). There were no significant differences between the two groups in other clinical outcomes such as anastomotic leak, surgical morbidity and length of hospital stay.</p><p><strong>Conclusions: </strong>RIPC demonstrated significantly reduced POI rates and TNF-α levels in colorectal surgery and could be a potential supportive strategy to promote less tissue trauma and thus enhance bowel recovery. Larger randomized controlled trials with standardized study protocols are needed to validate the results presented here.</p>","PeriodicalId":17983,"journal":{"name":"Langenbeck's Archives of Surgery","volume":"410 1","pages":"268"},"PeriodicalIF":1.8000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12420691/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Langenbeck's Archives of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00423-025-03864-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Remote ischaemic preconditioning (RIPC) which consists of repeated brief episodes of non-lethal limb ischaemia is associated with organ protection and improved clinical outcomes through complex pathophysiological pathways. The aim of this meta-analysis was to evaluate the postoperative effects of RIPC in bowel recovery and surgical morbidity after colorectal surgery.
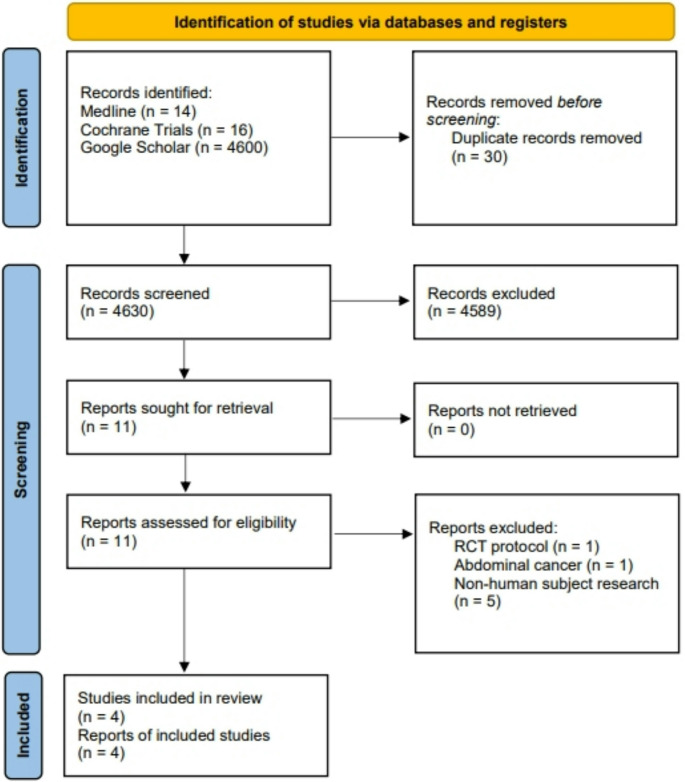
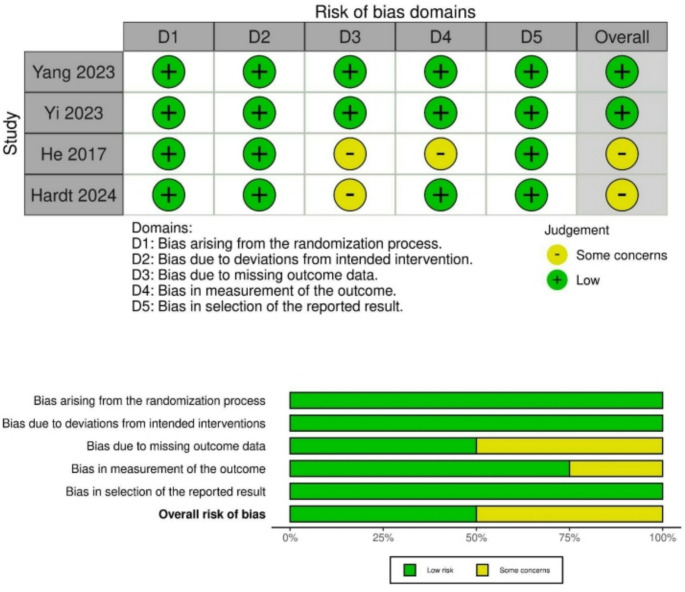
Methods: In strict adherence to the PRISMA guidelines, a systematic literature search was performed for studies comparing the postoperative effect RIPC in colorectal surgery. Data from eligible studies were extracted, qualitatively assessed, and included. Odds ratios (OR) and standardized mean differences (SMDs) with 95% confidence intervals (CIs) were calculated.
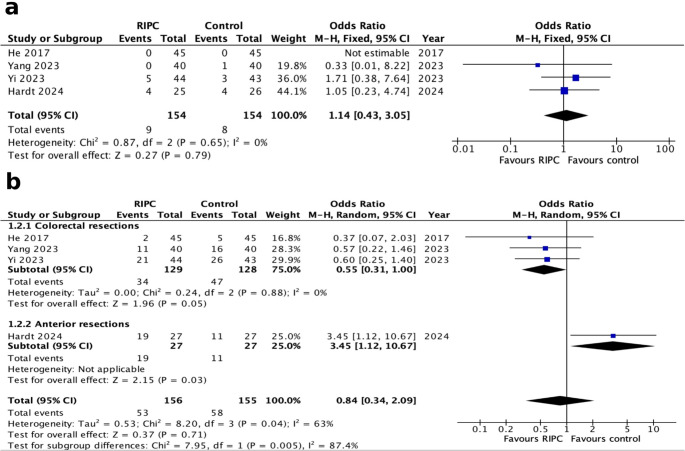
Results: Four studies with a total of 311 patients were included. RIPC resulted in reduced rates of postoperative ileus (POI) (OR 0.42, 95% CI 0.21-0.85, p = 0.02) and lower postoperative TNF-α levels (SMD - 1.01, 95% CI -1.59,-0.43, p = 0.0007). There were no significant differences between the two groups in other clinical outcomes such as anastomotic leak, surgical morbidity and length of hospital stay.
Conclusions: RIPC demonstrated significantly reduced POI rates and TNF-α levels in colorectal surgery and could be a potential supportive strategy to promote less tissue trauma and thus enhance bowel recovery. Larger randomized controlled trials with standardized study protocols are needed to validate the results presented here.
远程缺血预处理(RIPC)由反复短暂的非致死性肢体缺血发作组成,通过复杂的病理生理途径与器官保护和改善临床结果相关。本荟萃分析的目的是评估RIPC在结直肠癌术后肠道恢复和手术发病率方面的术后效果。方法:在严格遵循PRISMA指南的前提下,系统检索文献,比较RIPC在结直肠手术中的术后效果。从符合条件的研究中提取数据,进行定性评估并纳入。计算比值比(OR)和95%置信区间(ci)的标准化平均差(SMDs)。结果:纳入4项研究,共纳入311例患者。RIPC降低了术后肠梗阻(POI)发生率(OR 0.42, 95% CI 0.21-0.85, p = 0.02),降低了术后TNF-α水平(SMD - 1.01, 95% CI -1.59,-0.43, p = 0.0007)。两组在吻合口漏、手术发生率、住院时间等其他临床指标上无显著差异。结论:RIPC在结直肠手术中可显著降低POI率和TNF-α水平,可能是一种潜在的支持策略,可减少组织创伤,从而增强肠道恢复。需要采用标准化研究方案的更大规模随机对照试验来验证本文的结果。
期刊介绍:
Langenbeck''s Archives of Surgery aims to publish the best results in the field of clinical surgery and basic surgical research. The main focus is on providing the highest level of clinical research and clinically relevant basic research. The journal, published exclusively in English, will provide an international discussion forum for the controlled results of clinical surgery. The majority of published contributions will be original articles reporting on clinical data from general and visceral surgery, while endocrine surgery will also be covered. Papers on basic surgical principles from the fields of traumatology, vascular and thoracic surgery are also welcome. Evidence-based medicine is an important criterion for the acceptance of papers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


