{"title":"Impact of a 24/7 on-site percutaneous coronary intervention team strategy on door-to-wire time.","authors":"Liang Wang, Xinglin Yang, Wei Wu, Ran Tian, Ming Yang, Yechen Han, Jianzhong Shen, Hao Qian, Fan Guo, Tengyue Zhang, Xueqing Zhu, Xiaofeng Jin, Chonghui Wang, Hongzhi Xie, Zhongjie Fan, Zhujun Shen, Jihai Liu, Zhanjie Zhang, Xiaojun Ma, Zhenyu Liu, Huadong Zhu","doi":"10.1136/bmjoq-2025-003386","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Current guidelines recommend that the door-to-wire (D2W) time should be <90 min in patients undergoing primary percutaneous coronary intervention (PCI) for ST-segment elevation myocardial infarction (STEMI). This study evaluated the effect of a 24/7 on-site PCI team strategy on the D2W time.</p><p><strong>Methods: </strong>In this single-centre, retrospective study, patients with STEMI undergoing primary PCI within 1 year before (control group, n=143) and 1 year after (intervention group, n=96) implementing a 24/7 on-site PCI team strategy were enrolled. This strategy required that the PCI team was always available in hospital to minimise the time required to make the catheterisation laboratory ready for PCI. The primary endpoint was the D2W time, and the secondary endpoints were the rate of delayed PCI (D2W time ≥90 min) and the on-site time of the PCI team members. Multivariate analysis was conducted to determine the independent predictors of delayed PCI in the intervention group.</p><p><strong>Results: </strong>The D2W time was shorter (52 vs 97 min, p<0.001), the rate of delayed PCI was lower (19.8% vs 55.2%, p<0.001), but the on-site time of the PCI team members (35 040 vs 9960 hours) was longer in the intervention group than in the control group. Time-to-obtain electrocardiogram >10 min (p=0.027) and time-to-make STEMI diagnosis >9 min (p<i>=</i>0.001) were independent predictors of delayed PCI after implementing the strategy.</p><p><strong>Conclusions: </strong>Implementing a 24/7 on-site PCI team strategy was associated with reductions in the D2W time and the rate of delayed PCI but an increase in the on-site time of the PCI team members.</p>","PeriodicalId":9052,"journal":{"name":"BMJ Open Quality","volume":"14 3","pages":""},"PeriodicalIF":1.6000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421147/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Quality","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjoq-2025-003386","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Current guidelines recommend that the door-to-wire (D2W) time should be <90 min in patients undergoing primary percutaneous coronary intervention (PCI) for ST-segment elevation myocardial infarction (STEMI). This study evaluated the effect of a 24/7 on-site PCI team strategy on the D2W time.
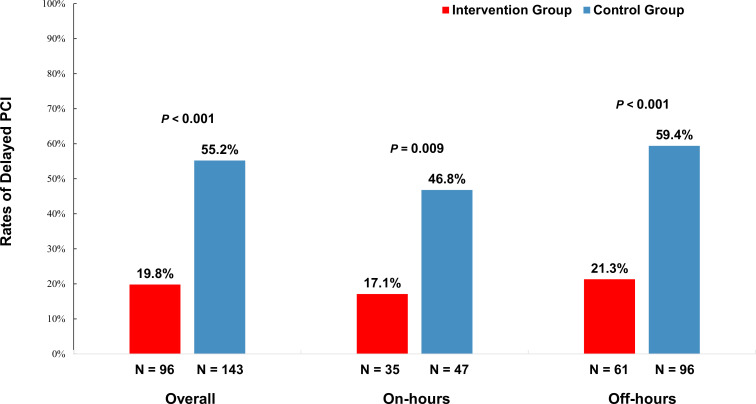
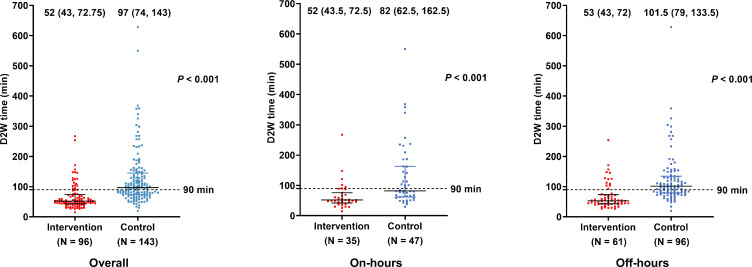
Methods: In this single-centre, retrospective study, patients with STEMI undergoing primary PCI within 1 year before (control group, n=143) and 1 year after (intervention group, n=96) implementing a 24/7 on-site PCI team strategy were enrolled. This strategy required that the PCI team was always available in hospital to minimise the time required to make the catheterisation laboratory ready for PCI. The primary endpoint was the D2W time, and the secondary endpoints were the rate of delayed PCI (D2W time ≥90 min) and the on-site time of the PCI team members. Multivariate analysis was conducted to determine the independent predictors of delayed PCI in the intervention group.
Results: The D2W time was shorter (52 vs 97 min, p<0.001), the rate of delayed PCI was lower (19.8% vs 55.2%, p<0.001), but the on-site time of the PCI team members (35 040 vs 9960 hours) was longer in the intervention group than in the control group. Time-to-obtain electrocardiogram >10 min (p=0.027) and time-to-make STEMI diagnosis >9 min (p=0.001) were independent predictors of delayed PCI after implementing the strategy.
Conclusions: Implementing a 24/7 on-site PCI team strategy was associated with reductions in the D2W time and the rate of delayed PCI but an increase in the on-site time of the PCI team members.
背景:目前的指南建议从门到线(D2W)的时间应该是:方法:在这项单中心回顾性研究中,STEMI患者在实施24/7现场PCI团队策略前1年(对照组,n=143)和1年后(干预组,n=96)接受了原发性PCI。该策略要求PCI团队始终在医院待命,以最大限度地减少导管实验室准备PCI所需的时间。主要终点为D2W时间,次要终点为PCI延迟率(D2W时间≥90 min)和PCI团队成员的现场时间。通过多因素分析确定干预组延迟PCI的独立预测因素。结果:D2W时间较短(52 vs 97 min, p10 min (p=0.027)和STEMI诊断时间bbb9 min (p=0.001)是实施该策略后延迟PCI的独立预测因子。结论:实施24/7现场PCI团队策略与减少D2W时间和延迟PCI率相关,但增加了PCI团队成员的现场时间。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


