Susan Mwikali Kioko, Christina Council, Cecilia Tomori
{"title":"Reducing Racial Disparities in Hypertension Control Using a Multicomponent, Equity-Centered Approach.","authors":"Susan Mwikali Kioko, Christina Council, Cecilia Tomori","doi":"10.1177/24731242251371424","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Black Americans have the highest prevalence of hypertension among all racial or ethnic groups in the United States. They are 40% more likely to have uncontrolled blood pressure (BP) and are five times more likely to die from hypertension compared with non-Hispanic Whites. Experiences of discrimination in health care, clinician and institutional bias, and socioeconomic and environmental inequities driven by structural racism contribute to uncontrolled hypertension in this population. Multilevel, multicomponent interventions have effectively improved BP control among Black Americans but remain inadequately implemented in the clinical setting. An integrated nursing/public health quality improvement study was designed to address this gap between evidence and integration into clinical practice.</p><p><strong>Methods: </strong>Using a one group pre/posttest design, we examined the effect of an innovative, evidence-based 12-week intervention on BP among Black Americans with uncontrolled hypertension aged 18 and older in the primary care setting. Intervention components included remote BP monitoring, weekly phone coaching with culturally congruent care, medication intensification, and a standardized hypertension protocol.</p><p><strong>Results: </strong>The average age of the participants (<i>n</i> = 35) was 64 years, and two thirds (<i>n</i> = 23) were female (66%). The mean difference in systolic BP from pre to postintervention decreased significantly (M = 23, standard deviation [SD] = 14.0), <i>t(34)</i> = -9.7, <i>p</i> < 0.001). A significant reduction in the mean difference in diastolic BP from pre to postintervention was also observed (M = 11, SD = 11.8), <i>t(34)</i> = -5.5, <i>p</i> < 0.001). At 12 weeks, 87% of participants had achieved BP control. The intervention also improved medication adherence and hypertension knowledge (<i>p</i> < 0.001).</p><p><strong>Conclusion: </strong>A multicomponent, culturally congruent quality improvement intervention may effectively improve BP among Black Americans.</p><p><strong>Health equity implications: </strong>Scaled up implementation of equity-centered, culturally congruent approaches is needed to reduce racial disparities in hypertension control.</p>","PeriodicalId":36602,"journal":{"name":"Health Equity","volume":"9 1","pages":"416-424"},"PeriodicalIF":2.5000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12412386/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Equity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24731242251371424","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Black Americans have the highest prevalence of hypertension among all racial or ethnic groups in the United States. They are 40% more likely to have uncontrolled blood pressure (BP) and are five times more likely to die from hypertension compared with non-Hispanic Whites. Experiences of discrimination in health care, clinician and institutional bias, and socioeconomic and environmental inequities driven by structural racism contribute to uncontrolled hypertension in this population. Multilevel, multicomponent interventions have effectively improved BP control among Black Americans but remain inadequately implemented in the clinical setting. An integrated nursing/public health quality improvement study was designed to address this gap between evidence and integration into clinical practice.
Methods: Using a one group pre/posttest design, we examined the effect of an innovative, evidence-based 12-week intervention on BP among Black Americans with uncontrolled hypertension aged 18 and older in the primary care setting. Intervention components included remote BP monitoring, weekly phone coaching with culturally congruent care, medication intensification, and a standardized hypertension protocol.
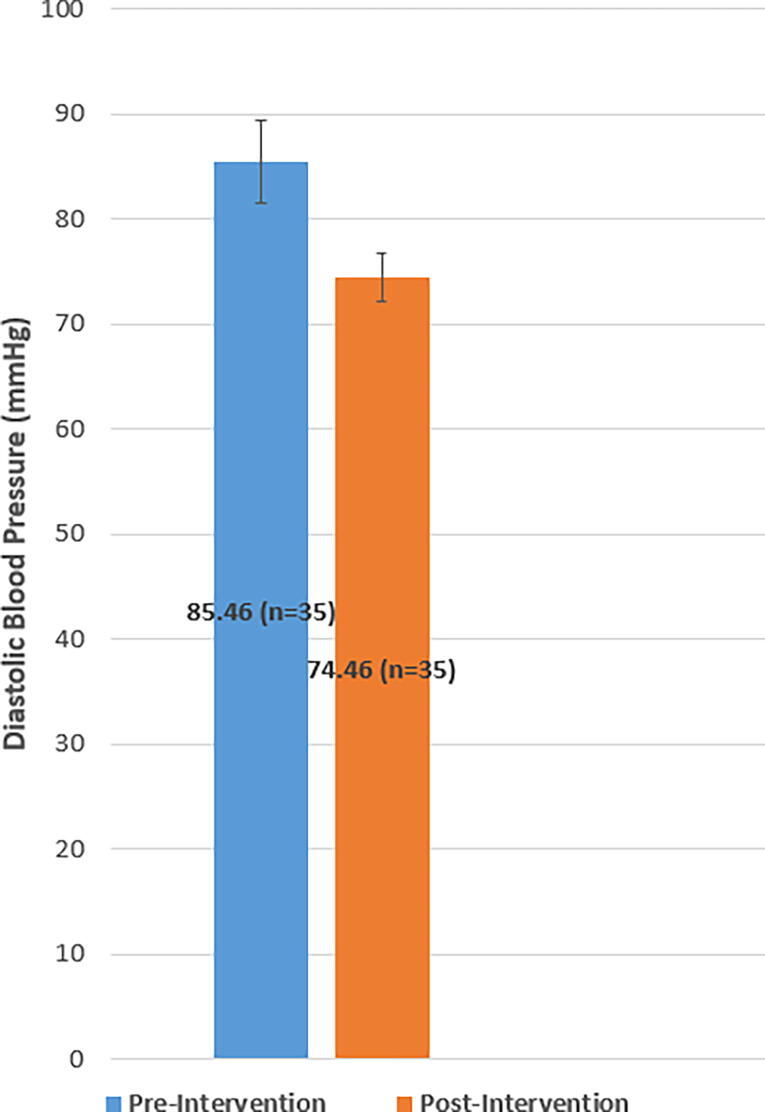
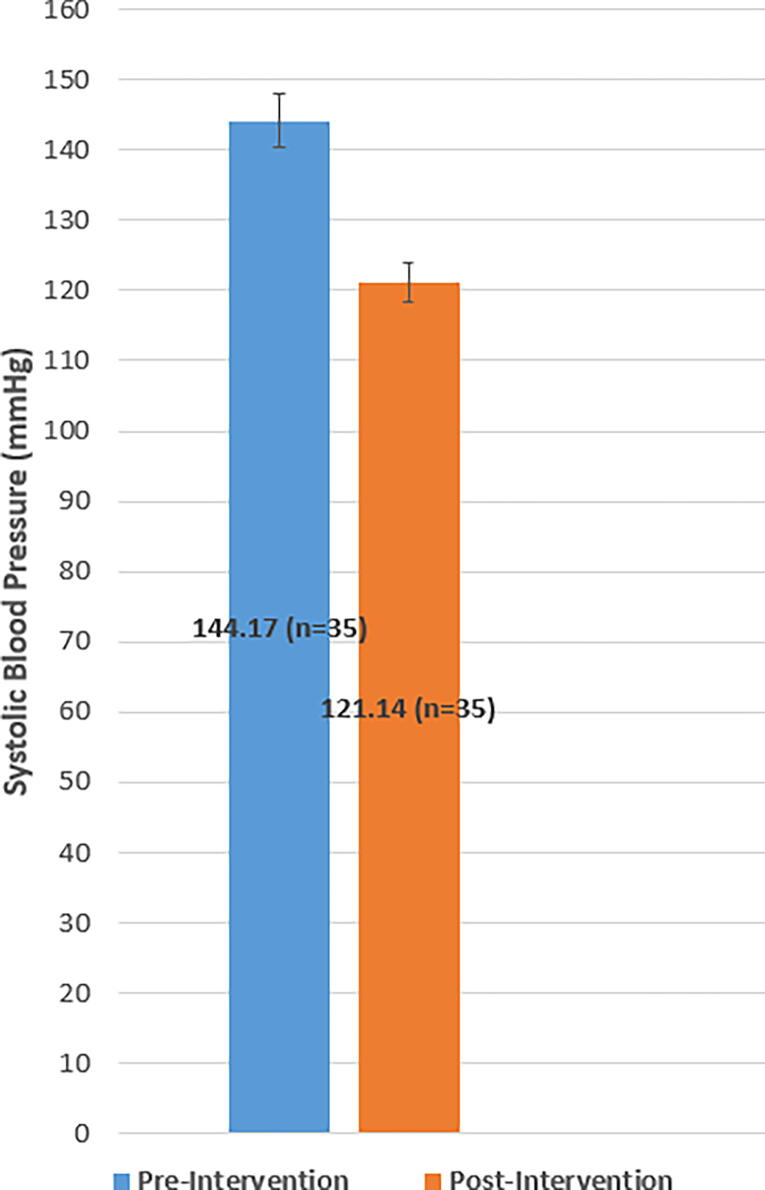
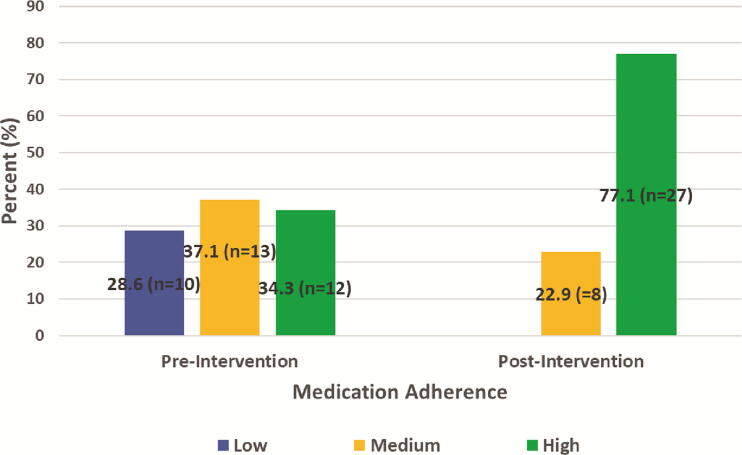
Results: The average age of the participants (n = 35) was 64 years, and two thirds (n = 23) were female (66%). The mean difference in systolic BP from pre to postintervention decreased significantly (M = 23, standard deviation [SD] = 14.0), t(34) = -9.7, p < 0.001). A significant reduction in the mean difference in diastolic BP from pre to postintervention was also observed (M = 11, SD = 11.8), t(34) = -5.5, p < 0.001). At 12 weeks, 87% of participants had achieved BP control. The intervention also improved medication adherence and hypertension knowledge (p < 0.001).
Conclusion: A multicomponent, culturally congruent quality improvement intervention may effectively improve BP among Black Americans.
Health equity implications: Scaled up implementation of equity-centered, culturally congruent approaches is needed to reduce racial disparities in hypertension control.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


