Management of Severe Ulcerative Colitis with Ambulatory Intravenous Corticosteroids (MOSAIC): A Treatment Approach to Avoid Hospitalization in Immunocompromised Patients.
Sabrina L Chen, Nicole Arima, Kendall Beck, Uma Mahadevan, Sara Lewin
{"title":"Management of Severe Ulcerative Colitis with Ambulatory Intravenous Corticosteroids (MOSAIC): A Treatment Approach to Avoid Hospitalization in Immunocompromised Patients.","authors":"Sabrina L Chen, Nicole Arima, Kendall Beck, Uma Mahadevan, Sara Lewin","doi":"10.1093/crocol/otaf053","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Acute severe ulcerative colitis (ASUC) typically requires hospitalization for intravenous (IV) corticosteroid treatment and monitoring. In response to the need to reduce inpatient stays, especially during the COVID-19 pandemic, outpatient treatment models have gained interest. This study evaluated the feasibility, safety, and patient satisfaction of outpatient IV corticosteroid treatment for ASUC.</p><p><strong>Methods: </strong>We conducted a prospective cohort feasibility pilot study at a single academic center between May 2021 and October 2022. Fifteen adults with ASUC were enrolled and self-selected either outpatient or inpatient IV corticosteroid treatment. All participants received daily laboratory monitoring and symptom assessments for 14 days, with follow-up for 1 year. Primary outcomes included 90-day colectomy and 30-day readmission rates. Secondary outcomes included clinical activity scores, symptom and care satisfaction, and feasibility metrics.</p><p><strong>Results: </strong>Ten patients received outpatient care, and 5 were hospitalized. No patients in either group required colectomy within 90 days. One outpatient and no inpatients required colectomy within 1 year. Thirty-day readmission occurred in 30% of outpatients and 40% of inpatients. Clinical activity scores and satisfaction with food and sleep were similar between groups at baseline and on day 14. Initial care satisfaction was lower in the outpatient group but equalized by day 14. Outpatient care required significant coordination but was successfully delivered without adverse safety outcomes.</p><p><strong>Discussion: </strong>Outpatient IV corticosteroid treatment for select patients with ASUC is feasible, safe, and associated with comparable clinical outcomes and patient satisfaction compared to inpatient care. This model may offer a cost-effective alternative to hospitalization.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"7 3","pages":"otaf053"},"PeriodicalIF":1.8000,"publicationDate":"2025-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12410984/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otaf053","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
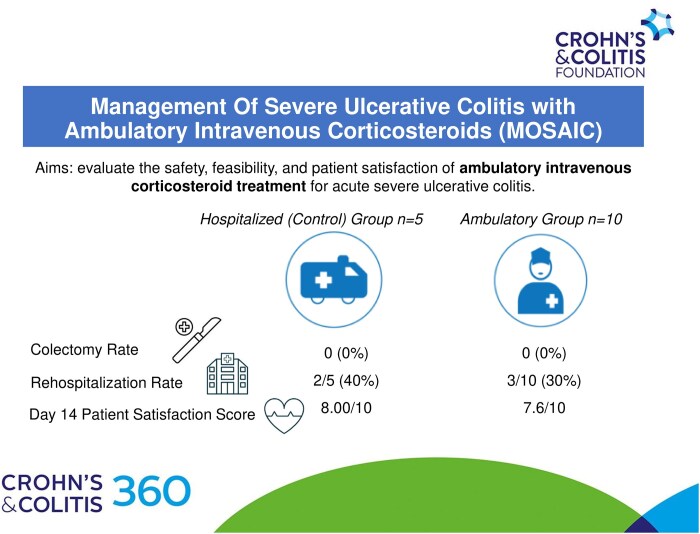
Introduction: Acute severe ulcerative colitis (ASUC) typically requires hospitalization for intravenous (IV) corticosteroid treatment and monitoring. In response to the need to reduce inpatient stays, especially during the COVID-19 pandemic, outpatient treatment models have gained interest. This study evaluated the feasibility, safety, and patient satisfaction of outpatient IV corticosteroid treatment for ASUC.
Methods: We conducted a prospective cohort feasibility pilot study at a single academic center between May 2021 and October 2022. Fifteen adults with ASUC were enrolled and self-selected either outpatient or inpatient IV corticosteroid treatment. All participants received daily laboratory monitoring and symptom assessments for 14 days, with follow-up for 1 year. Primary outcomes included 90-day colectomy and 30-day readmission rates. Secondary outcomes included clinical activity scores, symptom and care satisfaction, and feasibility metrics.
Results: Ten patients received outpatient care, and 5 were hospitalized. No patients in either group required colectomy within 90 days. One outpatient and no inpatients required colectomy within 1 year. Thirty-day readmission occurred in 30% of outpatients and 40% of inpatients. Clinical activity scores and satisfaction with food and sleep were similar between groups at baseline and on day 14. Initial care satisfaction was lower in the outpatient group but equalized by day 14. Outpatient care required significant coordination but was successfully delivered without adverse safety outcomes.
Discussion: Outpatient IV corticosteroid treatment for select patients with ASUC is feasible, safe, and associated with comparable clinical outcomes and patient satisfaction compared to inpatient care. This model may offer a cost-effective alternative to hospitalization.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


