Comparison of the Reverse Shock Index Multiplied by Glasgow Coma Scale Score, MEWS, and qSOFA as Sepsis Screening Tools for Predicting Short-Term Outcomes.
{"title":"Comparison of the Reverse Shock Index Multiplied by Glasgow Coma Scale Score, MEWS, and qSOFA as Sepsis Screening Tools for Predicting Short-Term Outcomes.","authors":"Wataru Matsuda, Akio Kimura, Tatsuki Uemura","doi":"10.2147/OAEM.S521868","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A simple screening tool is needed for resource-limited settings because rapid treatment is crucial in sepsis. We investigated whether a simplified score, the reverse shock index multiplied by the Glasgow Coma Scale score (rSIG), could replace the Modified Early Warning Score (MEWS) or the quick Sequential Organ Failure Assessment (qSOFA) for sepsis screening.</p><p><strong>Methods: </strong>We used data from a Japanese multicenter prospective observational study. This dataset included patients with suspected infection who were admitted from 35 emergency departments (cohort 1) and patients with suspected infection who were admitted to 22 intensive care units (cohort 2). The primary outcome was 28-day mortality. Secondary outcomes were ICU admission or death within 28 days and mechanical ventilation or death within 28 days in cohort 1 and diagnosis of sepsis, need for invasive support (composite of vasopressor use, mechanical ventilation, or death before day 4) in cohort 2.</p><p><strong>Results: </strong>In cohort 1, the AUROC for rSIG was significantly higher for 28-day mortality than for MEWS but not significantly different from that of qSOFA (0.69 [95% CI 0.64-0.74] vs 0.64 [0.59-0.69] vs 0.68 [0.63-0.72]). In cohort 2, the AUROC of rSIG for 28-day mortality was similar to that of MEWS and qSOFA (0.62 [0.56-0.68] vs 0.58 [0.52-0.64] vs 0.62 [0.56-0.67]). The AUROCs for diagnosis of sepsis, ICU admission or 28-day mortality, and mechanical ventilation or 28-day mortality were similar. The AUROC for need of invasive support was significantly higher for rSIG than for MEWS. For most outcomes, rSIG ≥15 had higher sensitivity than a qSOFA ≥2 or a MEWS total ≥5 or any variable ≥3.</p><p><strong>Conclusion: </strong>Although there are limitations in the data, rSIG predicted short-term outcomes in patients with suspected infections as well as or better than MEWS and qSOFA.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"17 ","pages":"247-255"},"PeriodicalIF":1.5000,"publicationDate":"2025-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413838/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S521868","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A simple screening tool is needed for resource-limited settings because rapid treatment is crucial in sepsis. We investigated whether a simplified score, the reverse shock index multiplied by the Glasgow Coma Scale score (rSIG), could replace the Modified Early Warning Score (MEWS) or the quick Sequential Organ Failure Assessment (qSOFA) for sepsis screening.
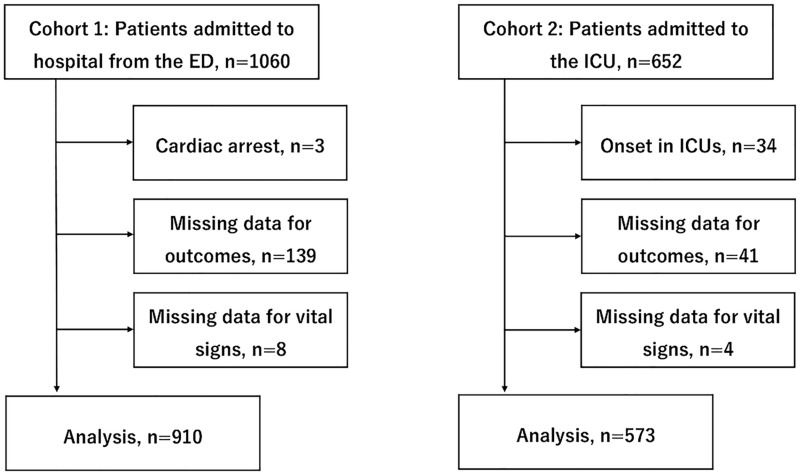
Methods: We used data from a Japanese multicenter prospective observational study. This dataset included patients with suspected infection who were admitted from 35 emergency departments (cohort 1) and patients with suspected infection who were admitted to 22 intensive care units (cohort 2). The primary outcome was 28-day mortality. Secondary outcomes were ICU admission or death within 28 days and mechanical ventilation or death within 28 days in cohort 1 and diagnosis of sepsis, need for invasive support (composite of vasopressor use, mechanical ventilation, or death before day 4) in cohort 2.
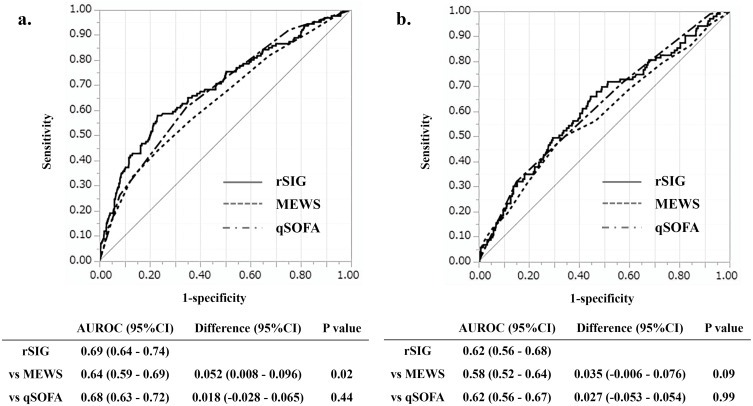
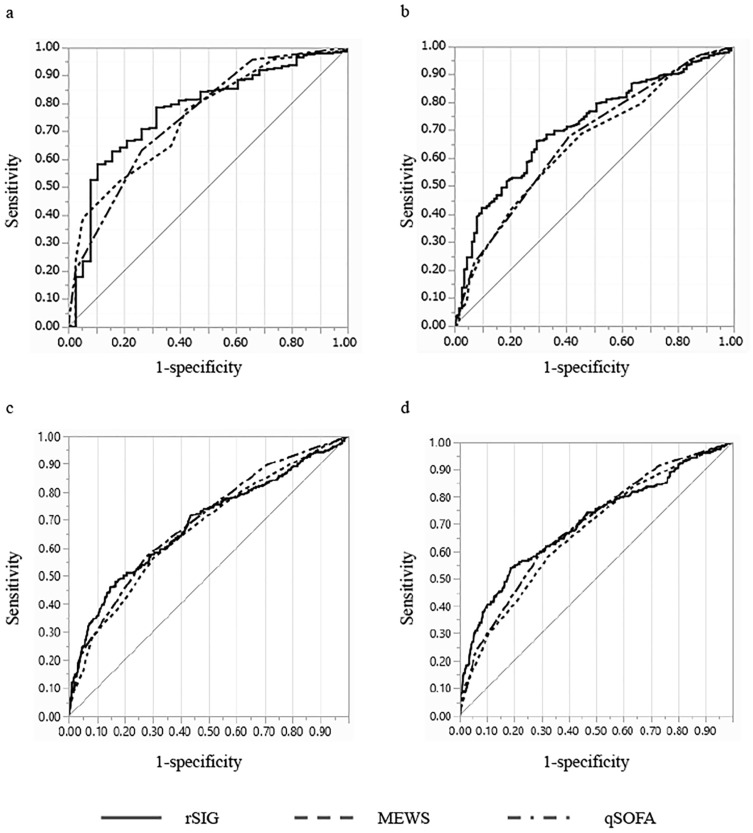
Results: In cohort 1, the AUROC for rSIG was significantly higher for 28-day mortality than for MEWS but not significantly different from that of qSOFA (0.69 [95% CI 0.64-0.74] vs 0.64 [0.59-0.69] vs 0.68 [0.63-0.72]). In cohort 2, the AUROC of rSIG for 28-day mortality was similar to that of MEWS and qSOFA (0.62 [0.56-0.68] vs 0.58 [0.52-0.64] vs 0.62 [0.56-0.67]). The AUROCs for diagnosis of sepsis, ICU admission or 28-day mortality, and mechanical ventilation or 28-day mortality were similar. The AUROC for need of invasive support was significantly higher for rSIG than for MEWS. For most outcomes, rSIG ≥15 had higher sensitivity than a qSOFA ≥2 or a MEWS total ≥5 or any variable ≥3.
Conclusion: Although there are limitations in the data, rSIG predicted short-term outcomes in patients with suspected infections as well as or better than MEWS and qSOFA.
背景:资源有限的环境需要一种简单的筛查工具,因为快速治疗对败血症至关重要。我们研究了一个简化的评分,即反向休克指数乘以格拉斯哥昏迷量表评分(rSIG),是否可以取代修改的早期预警评分(MEWS)或快速顺序器官衰竭评估(qSOFA),用于败血症筛查。方法:我们使用来自日本一项多中心前瞻性观察研究的数据。该数据集包括35个急诊科收治的疑似感染患者(队列1)和22个重症监护病房收治的疑似感染患者(队列2)。主要终点为28天死亡率。次要结局为队列1的28天内进入ICU或死亡、机械通气或28天内死亡;队列2的诊断为败血症、需要有创支持(使用血管加压剂、机械通气或第4天前死亡)。结果:在队列1中,rSIG的28天死亡率AUROC显著高于MEWS,但与qSOFA无显著差异(0.69 [95% CI 0.64-0.74] vs 0.64 [0.59-0.69] vs 0.68[0.63-0.72])。在队列2中,rSIG的28天死亡率AUROC与MEWS和qSOFA相似(0.62 [0.56-0.68]vs 0.58 [0.52-0.64] vs 0.62[0.56-0.67])。诊断败血症、ICU住院或28天死亡率、机械通气或28天死亡率的auroc相似。rSIG患者需要有创支持的AUROC显著高于MEWS患者。对于大多数结果,rSIG≥15比qSOFA≥2或MEWS总分≥5或任何变量≥3具有更高的敏感性。结论:尽管数据存在局限性,但rSIG预测疑似感染患者的短期预后与MEWS和qSOFA一样好,甚至更好。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


