{"title":"DLCO in HIV Patients and Their Association with CD4 and VL.","authors":"Tianjiao Xue, Tingting Liu, Yanfen Tang, Qi Chen, Yanyan Liu, Chenxi Cui, Chaohu Zhang, Jing Liu, Meng Zhang, Guifang Jin, Yuanyuan Zhang, Yu Wang","doi":"10.2147/HIV.S532629","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The advent of highly active antiretroviral therapy (HAART) has changed infection by human immunodeficiency virus (HIV) from an acute disease to a manageable chronic condition; however, pulmonary complications continue to affect patient quality of life. The goal of this research was to examine the link between CD4+ levels, viral load, and respiratory function in patients infected with HIV.</p><p><strong>Methods: </strong>Patients were grouped as HIV-infected and non-infected (1:2 ratio). The analysis included between-group comparisons of the post-bronchodilator FEV1, FVC, FEV1/FVC ratio, forced expiratory flows at various lung volumes (FEF75, FEF50, FEF75/25), and carbon monoxide diffusion capacity (DLCO). We analyzed CD4+ counts and viral load effects on lung function using stepwise regression. For normally distributed continuous variables (presented as means ± SD), intergroup comparisons were performed using independent two-sample <i>t</i>-tests. Non-normal distributions (reported as medians [IQR]) were analyzed with Mann-Whitney <i>U</i>-tests. Categorical variables were compared using χ² or Fisher's exact tests, with statistical significance set at p < 0.05.</p><p><strong>Results: </strong>The study enrolled 150 participants infected with HIV with a mean age of 48 (39.25, 57.75) years; 87.33% were male and 46% had a history of smoking. The DLCO was significantly lower in patients with HIV (69.37 vs 82.23, p < 0.05) compared to patients without HIV. In patients with HIV, the DLCO was positively correlated with CD4+ T lymphocyte counts (r=0.5521, p < 0.0001) and negatively correlated with the HIV viral load (r=-0.3942, p < 0.0001), and both were statistically significant. Patients with CD4+ ≥ 200 cells/μL had significantly higher VC (89.52 vs 79.31), FVC (91.80 vs 83.55), FEV1 (91.60 vs 84.40), and DLCO (74.61 vs 57.96) than those with CD4+ < 200 cells/μL. Similarly, patients with undetectable viral loads had higher VC (87.99 vs 81.08), FVC (90.90 vs 83.70), and DLCO (72.59 vs 60.62) than those with detectable viremia (all p < 0.05). The CD4+ count and FVC were significant predictors of the DLCO (p < 0.05).</p><p><strong>Conclusion: </strong>HIV infection is significantly associated with impaired pulmonary diffusion function. Even after antiviral therapy when the viral load becomes undetectable (CD4+ T lymphocytes > 400), the impairment of pulmonary diffusion still persists. Therefore, we should strengthen the pulmonary function testing for AIDS patients, detect the risk of lung injury as early as possible, carry out timely interventions, and reduce the risk of chronic obstructive pulmonary disease (COPD).</p>","PeriodicalId":46555,"journal":{"name":"HIV AIDS-Research and Palliative Care","volume":"17 ","pages":"277-285"},"PeriodicalIF":1.8000,"publicationDate":"2025-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413822/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HIV AIDS-Research and Palliative Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/HIV.S532629","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The advent of highly active antiretroviral therapy (HAART) has changed infection by human immunodeficiency virus (HIV) from an acute disease to a manageable chronic condition; however, pulmonary complications continue to affect patient quality of life. The goal of this research was to examine the link between CD4+ levels, viral load, and respiratory function in patients infected with HIV.
Methods: Patients were grouped as HIV-infected and non-infected (1:2 ratio). The analysis included between-group comparisons of the post-bronchodilator FEV1, FVC, FEV1/FVC ratio, forced expiratory flows at various lung volumes (FEF75, FEF50, FEF75/25), and carbon monoxide diffusion capacity (DLCO). We analyzed CD4+ counts and viral load effects on lung function using stepwise regression. For normally distributed continuous variables (presented as means ± SD), intergroup comparisons were performed using independent two-sample t-tests. Non-normal distributions (reported as medians [IQR]) were analyzed with Mann-Whitney U-tests. Categorical variables were compared using χ² or Fisher's exact tests, with statistical significance set at p < 0.05.
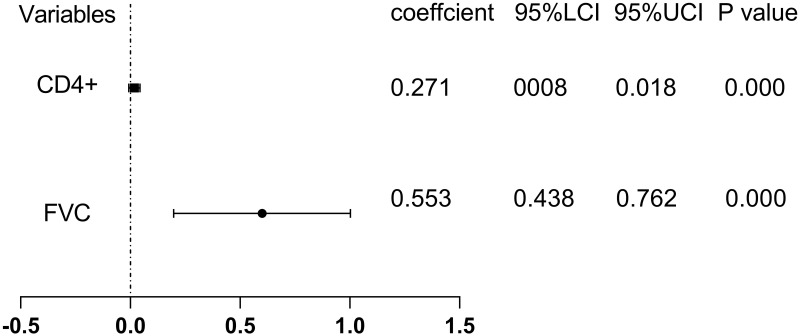
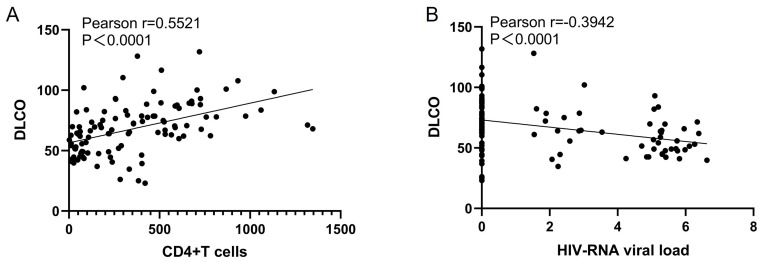
Results: The study enrolled 150 participants infected with HIV with a mean age of 48 (39.25, 57.75) years; 87.33% were male and 46% had a history of smoking. The DLCO was significantly lower in patients with HIV (69.37 vs 82.23, p < 0.05) compared to patients without HIV. In patients with HIV, the DLCO was positively correlated with CD4+ T lymphocyte counts (r=0.5521, p < 0.0001) and negatively correlated with the HIV viral load (r=-0.3942, p < 0.0001), and both were statistically significant. Patients with CD4+ ≥ 200 cells/μL had significantly higher VC (89.52 vs 79.31), FVC (91.80 vs 83.55), FEV1 (91.60 vs 84.40), and DLCO (74.61 vs 57.96) than those with CD4+ < 200 cells/μL. Similarly, patients with undetectable viral loads had higher VC (87.99 vs 81.08), FVC (90.90 vs 83.70), and DLCO (72.59 vs 60.62) than those with detectable viremia (all p < 0.05). The CD4+ count and FVC were significant predictors of the DLCO (p < 0.05).
Conclusion: HIV infection is significantly associated with impaired pulmonary diffusion function. Even after antiviral therapy when the viral load becomes undetectable (CD4+ T lymphocytes > 400), the impairment of pulmonary diffusion still persists. Therefore, we should strengthen the pulmonary function testing for AIDS patients, detect the risk of lung injury as early as possible, carry out timely interventions, and reduce the risk of chronic obstructive pulmonary disease (COPD).
高活性抗逆转录病毒疗法(HAART)的出现使人类免疫缺陷病毒(HIV)感染从一种急性疾病转变为一种可控制的慢性疾病;然而,肺部并发症继续影响患者的生活质量。这项研究的目的是检查CD4+水平、病毒载量和艾滋病毒感染者呼吸功能之间的联系。方法:将患者按1:2的比例分为hiv感染者和非感染者。分析包括支气管扩张剂后FEV1、FVC、FEV1/FVC比值、不同肺容积(FEF75、FEF50、FEF75/25)下用力呼气流量和一氧化碳扩散能力(DLCO)的组间比较。我们使用逐步回归分析了CD4+计数和病毒载量对肺功能的影响。对于正态分布的连续变量(以均数±SD表示),采用独立的双样本t检验进行组间比较。非正态分布(报告为中位数[IQR])采用Mann-Whitney u检验进行分析。分类变量比较采用χ 2或Fisher精确检验,p < 0.05为统计学显著性。结果:该研究纳入了150名HIV感染者,平均年龄48岁(39.25岁,57.75岁);87.33%为男性,46%有吸烟史。与未感染HIV的患者相比,HIV患者DLCO显著降低(69.37 vs 82.23, p < 0.05)。在HIV患者中,DLCO与CD4+ T淋巴细胞计数呈正相关(r=0.5521, p < 0.0001),与HIV病毒载量负相关(r=-0.3942, p < 0.0001),两者均有统计学意义。CD4+≥200 cells/μL患者的VC (89.52 vs 79.31)、FVC (91.80 vs 83.55)、FEV1 (91.60 vs 84.40)、DLCO (74.61 vs 57.96)均显著高于CD4+ < 200 cells/μL患者。同样,病毒载量检测不到的患者的VC (87.99 vs 81.08)、FVC (90.90 vs 83.70)和DLCO (72.59 vs 60.62)高于病毒载量检测到的患者(均p < 0.05)。CD4+计数和FVC是DLCO的显著预测因子(p < 0.05)。结论:HIV感染与肺弥散功能受损有显著相关性。即使经过抗病毒治疗,当病毒载量变得无法检测(CD4+ T淋巴细胞bbb400)时,肺扩散的损害仍然存在。因此,我们应该加强对艾滋病患者的肺功能检测,尽早发现肺损伤的危险,及时进行干预,降低慢性阻塞性肺疾病(COPD)的风险。
期刊介绍:
About Dove Medical Press Dove Medical Press Ltd is part of Taylor & Francis Group, the Academic Publishing Division of Informa PLC. We specialize in the publication of Open Access peer-reviewed journals across the broad spectrum of science, technology and especially medicine. Dove Medical Press was founded in 2003 with the objective of combining the highest editorial standards with the ''best of breed'' new publishing technologies. We have offices in Manchester and London in the United Kingdom, representatives in Princeton, New Jersey in the United States, and our editorial offices are in Auckland, New Zealand. Dr Scott Fraser is our Medical Director based in the UK. He has been in full time clinical practice for over 20 years as well as having an active research interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


