{"title":"Hemodynamic Effects of Guideline-Based Sedation in Mechanically Ventilated Adults: A Multicenter Observational Analysis.","authors":"Kiyan Heybati, Guozhen Xie, Jiawen Deng, Allan J Walkey, Ognjen Gajic, Hemang Yadav","doi":"10.1097/CCE.0000000000001313","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Propofol is a first-line sedative for adults receiving invasive mechanical ventilation (IMV). However, it can contribute to hemodynamic instability, especially during intubation. The magnitude, timing, risk factors, and variability of sedation-associated mean arterial pressure (MAP) changes remain poorly characterized in ICU settings.</p><p><strong>Objectives: </strong>To quantify MAP changes following propofol sedation, identify risk factors for hemodynamic instability, and characterize associated interventions.</p><p><strong>Design: </strong>Retrospective cohort study. The primary outcome was MAP change within 2 hours following sedation. Secondary outcomes included vasopressor use and hypotension (MAP ≤ 60 mm Hg). Mixed-effects modeling was used to account for individual patient differences.</p><p><strong>Setting and participants: </strong>Adults (≥ 18 yrs old) who required IMV and received greater than or equal to 6 consecutive hours of propofol infusion, between May 5th, 2018, and July 31st, 2024, in 11 ICUs across the Mayo Clinic, spanning 5 hospitals in 4 states.</p><p><strong>Main outcomes and measures: </strong>The primary outcome was the change in MAP within 2 hours following the initiation of propofol-based sedation.</p><p><strong>Results: </strong>Across 16,418 patients, 25.2% were on vasopressors before sedation initiation. Among the remaining 12,281 patients, 40.3% required vasopressors and 7.7% experienced hypotension within 2 hours of sedation. Propofol-based sedation was associated with a MAP reduction within the first 30 minutes (-6.58 mm Hg; 95% CI, -6.85 to -6.32; p < 0.001). There was substantial interpatient variability in both baseline MAP, and MAP decline after sedation (9.5 and 40.9% between-patient differences, respectively). Higher Sequential Organ Failure Assessment (SOFA) scores (-0.31 mm Hg/point), older age (-0.04 mm Hg/yr), and male sex (-0.47 mm Hg) were associated with lower MAP. Patients with higher illness severity experienced progressively greater MAP decline over time (-0.20 mm Hg/hr/SOFA point; p < 0.001).</p><p><strong>Conclusions and relevance: </strong>Propofol-based sedation was associated with clinically significant hemodynamic effects requiring intervention in the early post-intubation period. The marked interpatient variability in hemodynamic responses highlights the importance of personalized management approaches, including risk stratification based on age, sex, and illness severity.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 9","pages":"e1313"},"PeriodicalIF":2.7000,"publicationDate":"2025-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416995/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001313","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: Propofol is a first-line sedative for adults receiving invasive mechanical ventilation (IMV). However, it can contribute to hemodynamic instability, especially during intubation. The magnitude, timing, risk factors, and variability of sedation-associated mean arterial pressure (MAP) changes remain poorly characterized in ICU settings.
Objectives: To quantify MAP changes following propofol sedation, identify risk factors for hemodynamic instability, and characterize associated interventions.
Design: Retrospective cohort study. The primary outcome was MAP change within 2 hours following sedation. Secondary outcomes included vasopressor use and hypotension (MAP ≤ 60 mm Hg). Mixed-effects modeling was used to account for individual patient differences.
Setting and participants: Adults (≥ 18 yrs old) who required IMV and received greater than or equal to 6 consecutive hours of propofol infusion, between May 5th, 2018, and July 31st, 2024, in 11 ICUs across the Mayo Clinic, spanning 5 hospitals in 4 states.
Main outcomes and measures: The primary outcome was the change in MAP within 2 hours following the initiation of propofol-based sedation.
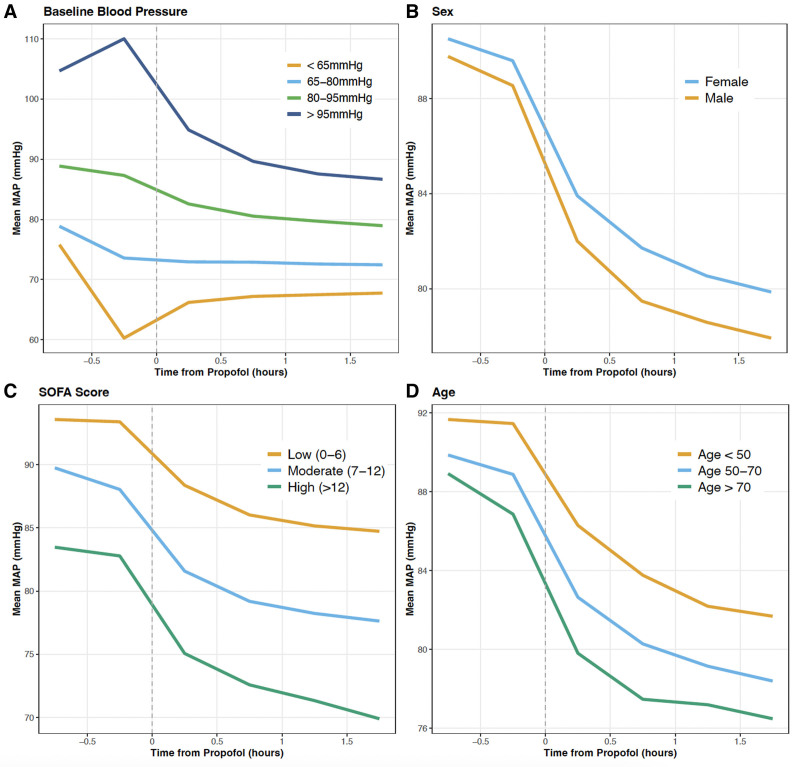
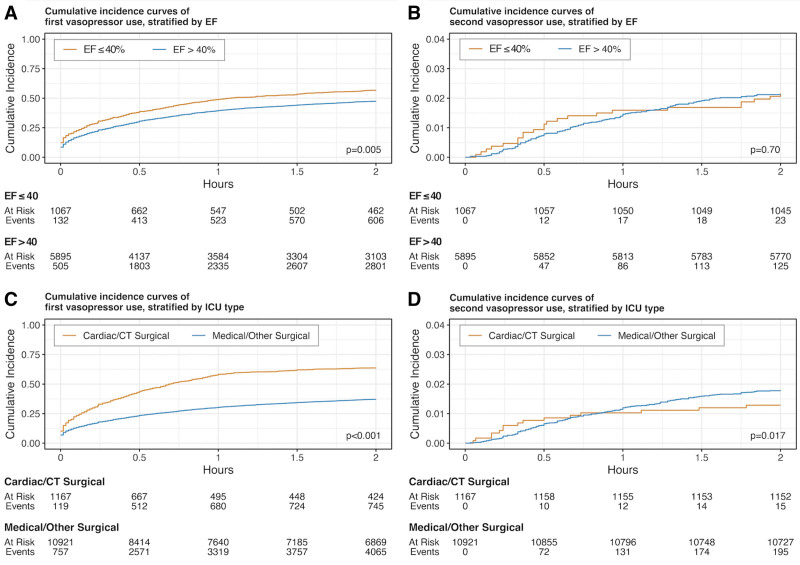
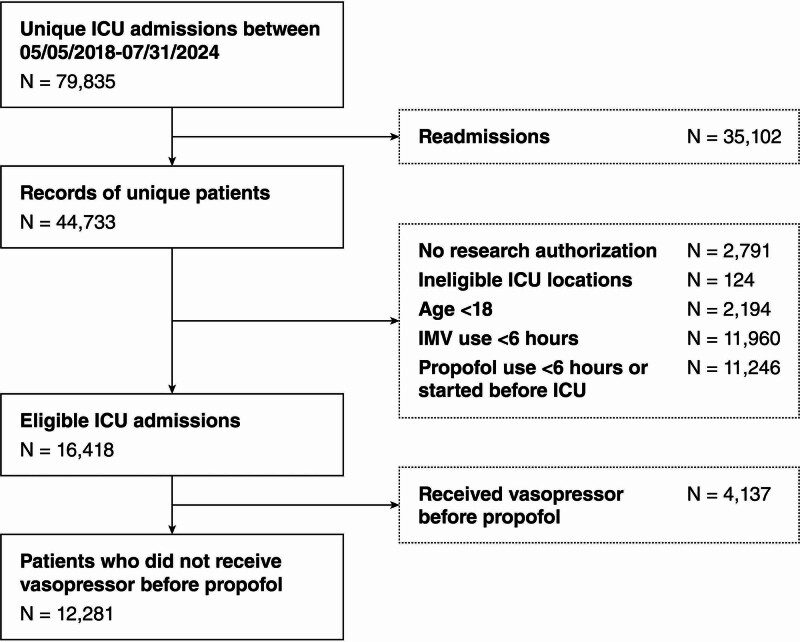
Results: Across 16,418 patients, 25.2% were on vasopressors before sedation initiation. Among the remaining 12,281 patients, 40.3% required vasopressors and 7.7% experienced hypotension within 2 hours of sedation. Propofol-based sedation was associated with a MAP reduction within the first 30 minutes (-6.58 mm Hg; 95% CI, -6.85 to -6.32; p < 0.001). There was substantial interpatient variability in both baseline MAP, and MAP decline after sedation (9.5 and 40.9% between-patient differences, respectively). Higher Sequential Organ Failure Assessment (SOFA) scores (-0.31 mm Hg/point), older age (-0.04 mm Hg/yr), and male sex (-0.47 mm Hg) were associated with lower MAP. Patients with higher illness severity experienced progressively greater MAP decline over time (-0.20 mm Hg/hr/SOFA point; p < 0.001).
Conclusions and relevance: Propofol-based sedation was associated with clinically significant hemodynamic effects requiring intervention in the early post-intubation period. The marked interpatient variability in hemodynamic responses highlights the importance of personalized management approaches, including risk stratification based on age, sex, and illness severity.
重要性:异丙酚是接受有创机械通气(IMV)的成人的一线镇静剂。然而,它可能导致血流动力学不稳定,特别是在插管期间。在ICU环境中,镇静相关的平均动脉压(MAP)变化的幅度、时间、危险因素和可变性仍然缺乏特征。目的:量化异丙酚镇静后MAP的变化,确定血流动力学不稳定的危险因素,并确定相关干预措施的特征。设计:回顾性队列研究。主要终点是镇静后2小时内MAP的变化。次要结局包括使用血管加压剂和低血压(MAP≤60 mm Hg)。混合效应模型用于解释个体患者的差异。环境和参与者:2018年5月5日至2024年7月31日期间,在梅奥诊所横跨4个州5家医院的11个icu中,需要IMV并接受大于或等于连续6小时异丙酚输注的成年人(≥18岁)。主要结局和指标:主要结局为异丙酚镇静开始后2小时内MAP的变化。结果:在16,418例患者中,25.2%的患者在镇静开始前使用血管加压药物。在剩余的12281例患者中,40.3%需要血管加压药物,7.7%在镇静2小时内出现低血压。基于异丙酚的镇静与前30分钟内MAP降低相关(-6.58 mm Hg; 95% CI, -6.85至-6.32;p < 0.001)。镇静后基线MAP和MAP下降的患者间差异很大(患者间差异分别为9.5%和40.9%)。较高的顺序器官衰竭评估(SOFA)评分(-0.31 mm Hg/分)、年龄(-0.04 mm Hg/年)和男性(-0.47 mm Hg)与较低的MAP相关。随着时间的推移,病情严重程度越高的患者MAP下降越严重(-0.20 mm Hg/hr/SOFA点;p < 0.001)。结论及相关性:异丙酚镇静与临床显著的血流动力学影响相关,需要在插管后早期进行干预。患者血流动力学反应的显著差异突出了个性化管理方法的重要性,包括基于年龄、性别和疾病严重程度的风险分层。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


