Native T1 adds independent value for cardiovascular risk assessment beyond global longitudinal strain in an all-comers real-world clinical patient population.
Sören J Backhaus, Julia Treiber, Jan Sebastian Wolter, Steffen D Kriechbaum, Ulla Fischer, Andreas Schuster, Valentina O Puntmann, Eike Nagel, Samuel Sossalla, Andreas Rolf
{"title":"Native T1 adds independent value for cardiovascular risk assessment beyond global longitudinal strain in an all-comers real-world clinical patient population.","authors":"Sören J Backhaus, Julia Treiber, Jan Sebastian Wolter, Steffen D Kriechbaum, Ulla Fischer, Andreas Schuster, Valentina O Puntmann, Eike Nagel, Samuel Sossalla, Andreas Rolf","doi":"10.1093/ehjopen/oeaf109","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Deformation imaging remains underused for cardiovascular risk assessment. As tissue characterization has now been recognized as an additional assessment tool, we sought to investigate the significance of native T1 and extracellular volume (ECV) in an unselected clinical routine population.</p><p><strong>Methods and results: </strong>The single-centre, prospective cardiovascular magnetic resonance (CMR) registry included patients referred for clinical CMR. Left ventricle global longitudinal strain (GLS) was evaluated in long-axis views. Native T1 and ECV were assessed on septal, basal, or midventricular short-axis positions. Follow-up was conducted for primary (all-cause mortality and heart failure hospitalization) and secondary (all-cause mortality, hospitalized angina, and myocardial infarction) endpoints. The final population consisted of <i>n</i> = 1633 patients who met primary (<i>n</i> = 68) and secondary (<i>n</i> = 90) endpoints during the median follow-up of 395 days. A 10-ms T1 increase was associated with a hazard ratio (HR) of 1.11 [95% confidence interval (CI) 1.07-1.15, <i>P</i> < 0.001] for the primary endpoint independent of ECV (<i>P</i> = 0.738). T1 (HR 1.07, 95% CI 1.03-1.11, <i>P</i> = 0.001) but not ECV (<i>P</i> = 0.674) was an independent predictor for the primary endpoint after correction for common risk factors including age, New York Heart Association class, biomarker NT-proBNP/glomerular filtration rate, and GLS. After dichotomization at the median of 1126 ms, T1 added incremental value for primary endpoint prediction on Kaplan-Meier plots in patients with left ventricular ejection fraction above/below (<i>P</i> = 0.019/0.017) the median of 55% and GLS above/below (<i>P</i> = 0.019/0.041) the median of -16.4%.</p><p><strong>Conclusion: </strong>Native T1 was found to be an independent risk predictor beyond GLS as well as common clinical risk factors. This may justify the use of non-contrast CMR protocols in selected patients if contrast application is contraindicated.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 5","pages":"oeaf109"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12405752/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf109","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Deformation imaging remains underused for cardiovascular risk assessment. As tissue characterization has now been recognized as an additional assessment tool, we sought to investigate the significance of native T1 and extracellular volume (ECV) in an unselected clinical routine population.
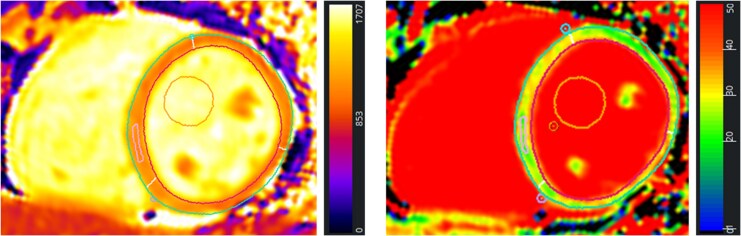
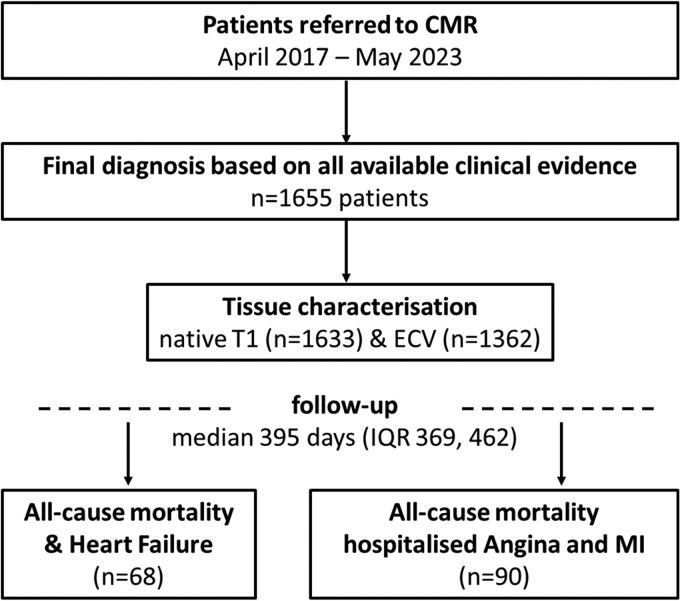
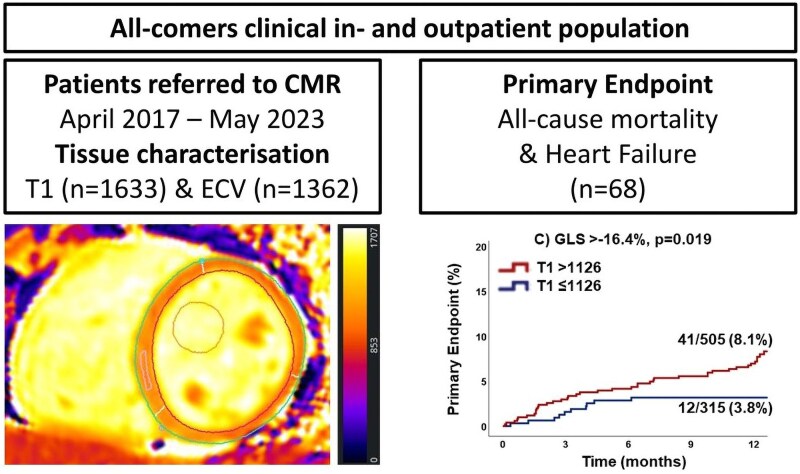
Methods and results: The single-centre, prospective cardiovascular magnetic resonance (CMR) registry included patients referred for clinical CMR. Left ventricle global longitudinal strain (GLS) was evaluated in long-axis views. Native T1 and ECV were assessed on septal, basal, or midventricular short-axis positions. Follow-up was conducted for primary (all-cause mortality and heart failure hospitalization) and secondary (all-cause mortality, hospitalized angina, and myocardial infarction) endpoints. The final population consisted of n = 1633 patients who met primary (n = 68) and secondary (n = 90) endpoints during the median follow-up of 395 days. A 10-ms T1 increase was associated with a hazard ratio (HR) of 1.11 [95% confidence interval (CI) 1.07-1.15, P < 0.001] for the primary endpoint independent of ECV (P = 0.738). T1 (HR 1.07, 95% CI 1.03-1.11, P = 0.001) but not ECV (P = 0.674) was an independent predictor for the primary endpoint after correction for common risk factors including age, New York Heart Association class, biomarker NT-proBNP/glomerular filtration rate, and GLS. After dichotomization at the median of 1126 ms, T1 added incremental value for primary endpoint prediction on Kaplan-Meier plots in patients with left ventricular ejection fraction above/below (P = 0.019/0.017) the median of 55% and GLS above/below (P = 0.019/0.041) the median of -16.4%.
Conclusion: Native T1 was found to be an independent risk predictor beyond GLS as well as common clinical risk factors. This may justify the use of non-contrast CMR protocols in selected patients if contrast application is contraindicated.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


