Karen Mulligan, Drishti Baid, Maria-Alice Manetas, Darius N Lakdawalla
{"title":"Measuring the Budget Impact of Nondiscriminatory Cost-Effectiveness.","authors":"Karen Mulligan, Drishti Baid, Maria-Alice Manetas, Darius N Lakdawalla","doi":"10.1001/jamahealthforum.2025.3076","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>The US Inflation and Reduction Act (IRA) prohibits the Centers for Medicare & Medicaid Services (CMS) from using discriminatory methods such as cost-effectiveness analysis (CEA) that assign lower value to treating sicker and disabled persons. Generalized risk-adjusted cost- effectiveness (GRACE) provides a nondiscriminatory alternative, but the potential impact on health care budgets is unknown.</p><p><strong>Objective: </strong>To compare value-based drug prices based on traditional CEA with those based on IRA-compliant GRACE and assess the implications for health care budgets.</p><p><strong>Design and setting: </strong>In this economic evaluation, GRACE was implemented using the direct-utility method and estimated the resulting value-based prices and total budget impact. Model inputs were derived from CEAs published by the Institute for Clinical and Economic Review (ICER) between 2014 and 2024. Data from 302 CEA results for pharmaceuticals published across 72 studies were extracted. The final analysis sample consisted of 259 observations (219 treatment-comparator pairs) across 53 distinct diseases, some of which had subgroup results.</p><p><strong>Main outcomes and measures: </strong>Value-based prices under GRACE and CEA were estimated. A 1-year budget impact was calculated, measured as total drug expenditures using value-based prices assuming a willingness-to-pay threshold of $150 000. The data were analyzed from October 2024 to May 2025.</p><p><strong>Results: </strong>The mean value-based prices were 7.5% higher under GRACE than under CEA (IQR, -3.9% to 9.1%). Furthermore, compared with traditional CEA, GRACE increased value-based prices for more severe diseases and decreased them for milder diseases. Twenty-four drugs (8 from the top population size quartile) cost less under GRACE; total spending was 3.3% lower under GRACE for these drugs. The remaining 45 drugs (13 from the bottom population size quartile) cost more under GRACE, resulting in 14.7% higher spending for these drugs. Taken together, GRACE increased the total budget by 2%..</p><p><strong>Conclusions and relevance: </strong>This economic evaluation found that although GRACE does increase value-based prices on average, the net effect on total health care spent is minimal, in part because resources are redistributed toward more severe, less prevalent illnesses.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"6 9","pages":"e253076"},"PeriodicalIF":11.3000,"publicationDate":"2025-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413641/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2025.3076","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: The US Inflation and Reduction Act (IRA) prohibits the Centers for Medicare & Medicaid Services (CMS) from using discriminatory methods such as cost-effectiveness analysis (CEA) that assign lower value to treating sicker and disabled persons. Generalized risk-adjusted cost- effectiveness (GRACE) provides a nondiscriminatory alternative, but the potential impact on health care budgets is unknown.
Objective: To compare value-based drug prices based on traditional CEA with those based on IRA-compliant GRACE and assess the implications for health care budgets.
Design and setting: In this economic evaluation, GRACE was implemented using the direct-utility method and estimated the resulting value-based prices and total budget impact. Model inputs were derived from CEAs published by the Institute for Clinical and Economic Review (ICER) between 2014 and 2024. Data from 302 CEA results for pharmaceuticals published across 72 studies were extracted. The final analysis sample consisted of 259 observations (219 treatment-comparator pairs) across 53 distinct diseases, some of which had subgroup results.
Main outcomes and measures: Value-based prices under GRACE and CEA were estimated. A 1-year budget impact was calculated, measured as total drug expenditures using value-based prices assuming a willingness-to-pay threshold of $150 000. The data were analyzed from October 2024 to May 2025.
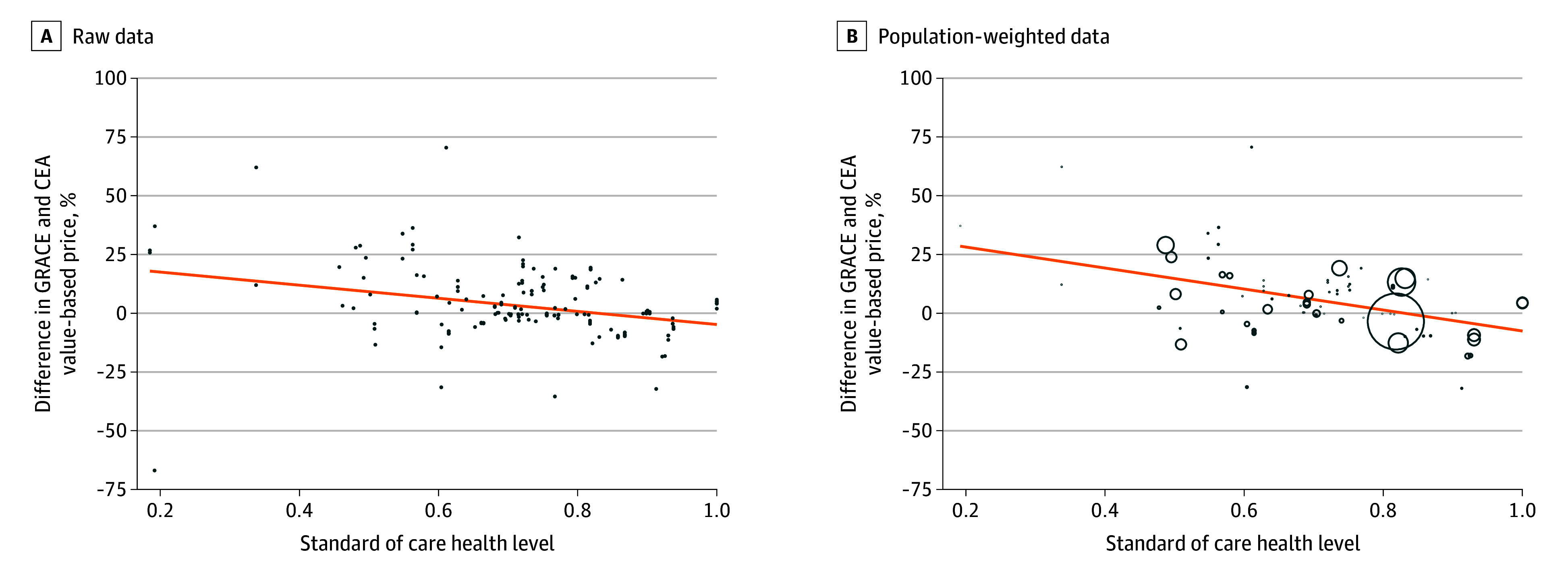
Results: The mean value-based prices were 7.5% higher under GRACE than under CEA (IQR, -3.9% to 9.1%). Furthermore, compared with traditional CEA, GRACE increased value-based prices for more severe diseases and decreased them for milder diseases. Twenty-four drugs (8 from the top population size quartile) cost less under GRACE; total spending was 3.3% lower under GRACE for these drugs. The remaining 45 drugs (13 from the bottom population size quartile) cost more under GRACE, resulting in 14.7% higher spending for these drugs. Taken together, GRACE increased the total budget by 2%..
Conclusions and relevance: This economic evaluation found that although GRACE does increase value-based prices on average, the net effect on total health care spent is minimal, in part because resources are redistributed toward more severe, less prevalent illnesses.
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


