Kathryn Evans, Qian Li, Lu Zhang, Sandi Lam, Bronwyn Do Rego, Vanessa Danielson, Reginald Lassagne, Ariel Berger
{"title":"Healthcare Utilization and Cost in the Two Years Before Neuromodulation Implantation Among Medicaid Enrollees with Drug-Resistant Epilepsy.","authors":"Kathryn Evans, Qian Li, Lu Zhang, Sandi Lam, Bronwyn Do Rego, Vanessa Danielson, Reginald Lassagne, Ariel Berger","doi":"10.2147/CEOR.S551202","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Current treatment guidelines recommend consideration of neurostimulators and other alternative treatments to antiseizure medications in patients with drug-resistant epilepsy (DRE). This study assessed patterns of utilization and cost of healthcare services and prescription pharmacotherapies during the 2-year period before neurostimulator implantation among Medicaid enrollees with DRE.</p><p><strong>Methods: </strong>This retrospective, observational cohort study used healthcare claims and enrollment data obtained from the US Centers for Medicare and Medicaid Services. Medicaid enrollees who met study selection criteria (ie, evidence of DRE and neurostimulator implantation) between January 1, 2011, and December 31, 2020, were included. Those without antiseizure medication (ASM) dispenses within 12 months of their implantation date or continuous enrollment for the 24-month period before this date were excluded. Demographic/clinical characteristics, utilization and cost of healthcare services, and prescription pharmacotherapies were assessed over the 2-year period before implantation. Care was designated as all-cause or epilepsy-related; the latter was defined as all ASM dispenses and all claims for medical care (ie, inpatient or outpatient) with a diagnosis code (any position) of epilepsy.</p><p><strong>Results: </strong>In total, 2469 patients met the selection criteria. Mean age at implantation was 20.8 years. Comorbidities were common. Over the 2-year period before implantation, patients were prescribed a mean of 4.4 unique ASMs. Fifty-seven percent had at least one all-cause hospital admission, and 82.9% had at least one all-cause emergency department visit; corresponding epilepsy-related values were 55.3% and 66.1%. Less than half of patients received specific cranial imaging, including video electroencephalographs. Total mean all-cause healthcare costs were $117,013; epilepsy-related healthcare costs accounted for $48,169 (41.2%).</p><p><strong>Conclusion: </strong>Medicaid enrollees with DRE experience high use and cost of healthcare services and pharmacotherapy over the 2 years before neurostimulator implantation. Further research is needed to understand the impacts associated with broader access to specialized epilepsy care, such as cranial imaging and neurostimulators.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"17 ","pages":"571-583"},"PeriodicalIF":2.2000,"publicationDate":"2025-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12402825/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S551202","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Current treatment guidelines recommend consideration of neurostimulators and other alternative treatments to antiseizure medications in patients with drug-resistant epilepsy (DRE). This study assessed patterns of utilization and cost of healthcare services and prescription pharmacotherapies during the 2-year period before neurostimulator implantation among Medicaid enrollees with DRE.
Methods: This retrospective, observational cohort study used healthcare claims and enrollment data obtained from the US Centers for Medicare and Medicaid Services. Medicaid enrollees who met study selection criteria (ie, evidence of DRE and neurostimulator implantation) between January 1, 2011, and December 31, 2020, were included. Those without antiseizure medication (ASM) dispenses within 12 months of their implantation date or continuous enrollment for the 24-month period before this date were excluded. Demographic/clinical characteristics, utilization and cost of healthcare services, and prescription pharmacotherapies were assessed over the 2-year period before implantation. Care was designated as all-cause or epilepsy-related; the latter was defined as all ASM dispenses and all claims for medical care (ie, inpatient or outpatient) with a diagnosis code (any position) of epilepsy.
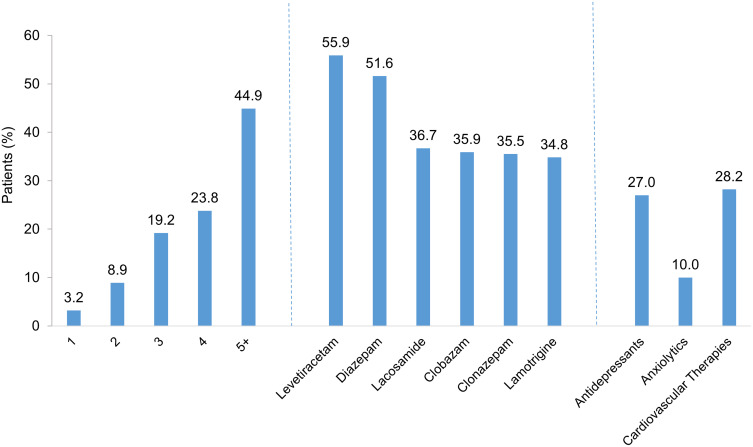
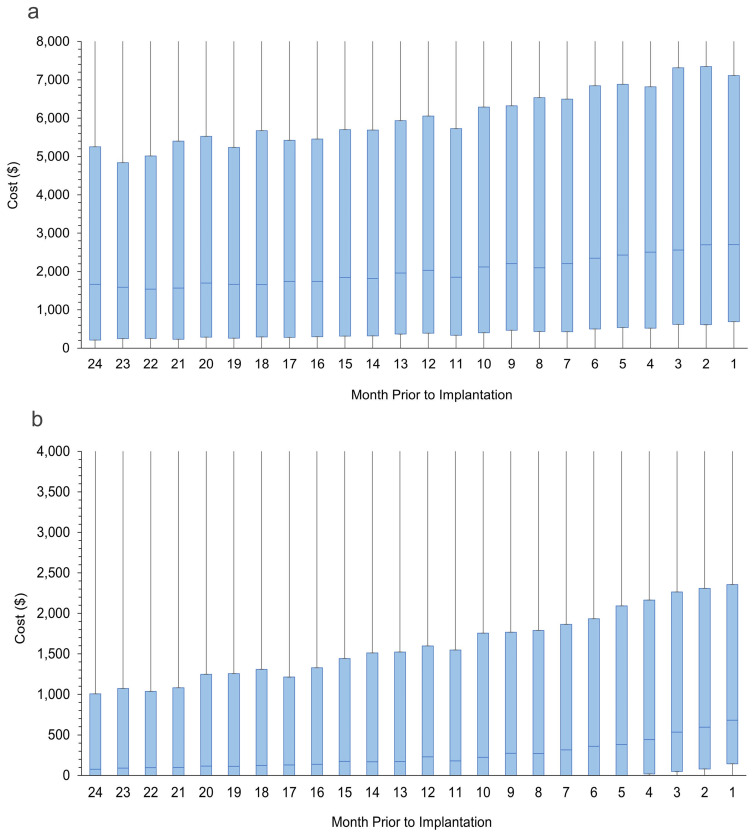
Results: In total, 2469 patients met the selection criteria. Mean age at implantation was 20.8 years. Comorbidities were common. Over the 2-year period before implantation, patients were prescribed a mean of 4.4 unique ASMs. Fifty-seven percent had at least one all-cause hospital admission, and 82.9% had at least one all-cause emergency department visit; corresponding epilepsy-related values were 55.3% and 66.1%. Less than half of patients received specific cranial imaging, including video electroencephalographs. Total mean all-cause healthcare costs were $117,013; epilepsy-related healthcare costs accounted for $48,169 (41.2%).
Conclusion: Medicaid enrollees with DRE experience high use and cost of healthcare services and pharmacotherapy over the 2 years before neurostimulator implantation. Further research is needed to understand the impacts associated with broader access to specialized epilepsy care, such as cranial imaging and neurostimulators.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


