Elizabeth Harris, Christian Rhudy, Lucas Roy, Amber Cloud, Christina Delacruz Leyson
{"title":"Sex differences in severity, outcomes, and healthcare utilization in alcohol-associated hepatitis.","authors":"Elizabeth Harris, Christian Rhudy, Lucas Roy, Amber Cloud, Christina Delacruz Leyson","doi":"10.4254/wjh.v17.i8.108063","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is increasing incidence of alcohol-associated liver disease in females. Despite this recent increased incidence, there is a paucity of research on the clinical course and outcomes of alcohol-associated hepatitis (AH) in females compared to males.</p><p><strong>Aim: </strong>To assess if there may be sex differences in severity, outcomes, and healthcare utilization for patients hospitalized for AH.</p><p><strong>Methods: </strong>This study used ICD-9-CM and ICD-10-CM codes to retrospectively identify inpatient encounters for AH at the University of Kentucky from 2012-2021 and obtained data on patient demographics and clinical outcomes. Encounters were cohorted by patient sex and differences in patient demographics and clinical outcomes were assessed. Multivariate logistic regression models were constructed to assess risk of mortality, sepsis, and mechanical ventilation during the encounter.</p><p><strong>Results: </strong>Of 1386 subjects, 511 (36.9%) were female and 875 (63.1%) were male. Both sexes had similar baseline characteristics of race/ethnicity, discriminant function score, model of end-stage liver disease score, and length of hospital stay. However, the incidence of urinary tract infection, sepsis, and norepinephrine administration was significantly higher for females. Males had a significantly higher incidence of esophageal variceal bleed. On multivariate logistic regression analysis, females had higher odds of encounter sepsis (OR 1.41; 95%CI: 1.064-1.869) and mechanical ventilation (OR 1.352; 95%CI: 1.006-1.816). Odds of encounter mortality were significantly increased in encounters with sepsis (OR 2.309; 95%CI: 1.419-3.757) and mechanical ventilation (OR 9.301; 95%CI: 5.724-15.114).</p><p><strong>Conclusion: </strong>This study shows sex-based differences in AH outcomes at the University of Kentucky. Future studies are warranted to assess whether tailoring treatments will improve clinical outcomes in females with AH.</p>","PeriodicalId":23687,"journal":{"name":"World Journal of Hepatology","volume":"17 8","pages":"108063"},"PeriodicalIF":2.5000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400398/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4254/wjh.v17.i8.108063","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There is increasing incidence of alcohol-associated liver disease in females. Despite this recent increased incidence, there is a paucity of research on the clinical course and outcomes of alcohol-associated hepatitis (AH) in females compared to males.
Aim: To assess if there may be sex differences in severity, outcomes, and healthcare utilization for patients hospitalized for AH.
Methods: This study used ICD-9-CM and ICD-10-CM codes to retrospectively identify inpatient encounters for AH at the University of Kentucky from 2012-2021 and obtained data on patient demographics and clinical outcomes. Encounters were cohorted by patient sex and differences in patient demographics and clinical outcomes were assessed. Multivariate logistic regression models were constructed to assess risk of mortality, sepsis, and mechanical ventilation during the encounter.
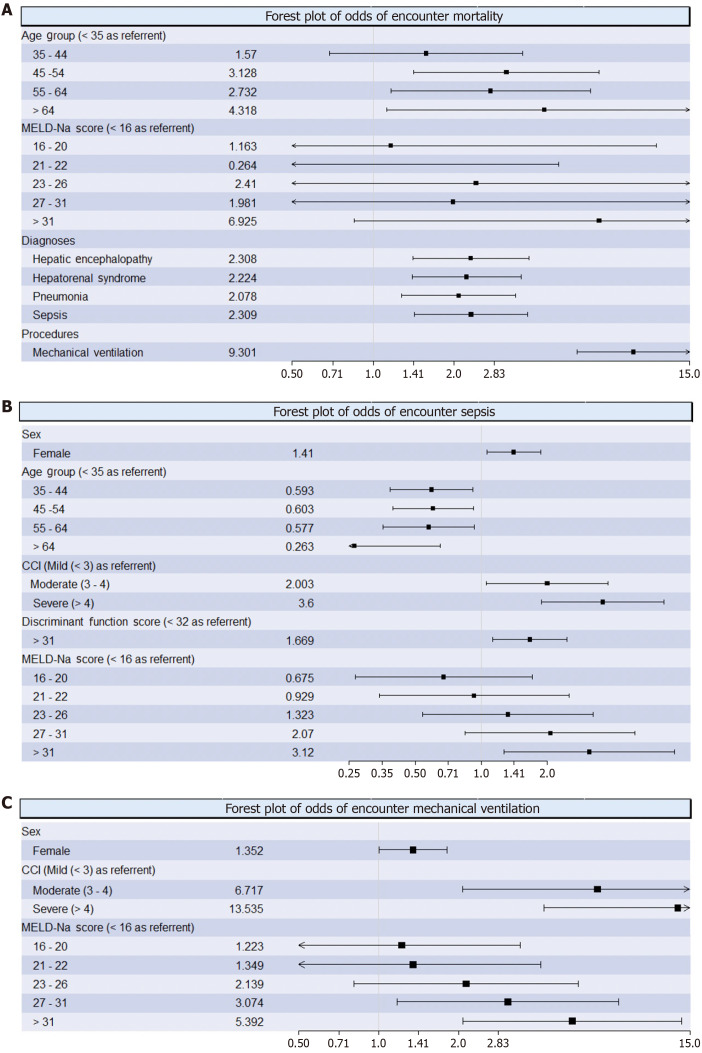
Results: Of 1386 subjects, 511 (36.9%) were female and 875 (63.1%) were male. Both sexes had similar baseline characteristics of race/ethnicity, discriminant function score, model of end-stage liver disease score, and length of hospital stay. However, the incidence of urinary tract infection, sepsis, and norepinephrine administration was significantly higher for females. Males had a significantly higher incidence of esophageal variceal bleed. On multivariate logistic regression analysis, females had higher odds of encounter sepsis (OR 1.41; 95%CI: 1.064-1.869) and mechanical ventilation (OR 1.352; 95%CI: 1.006-1.816). Odds of encounter mortality were significantly increased in encounters with sepsis (OR 2.309; 95%CI: 1.419-3.757) and mechanical ventilation (OR 9.301; 95%CI: 5.724-15.114).
Conclusion: This study shows sex-based differences in AH outcomes at the University of Kentucky. Future studies are warranted to assess whether tailoring treatments will improve clinical outcomes in females with AH.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


