Paul A Scott, Antonio Cannata, Daniel I Bromage, Ian J Wright, Anish Bhuva, Matthew J Lovell, Chris Plummer, Mark de Belder, Mark Dayer, Francis Murgatroyd
{"title":"Complications after complex device implantation: how important is implanter seniority?","authors":"Paul A Scott, Antonio Cannata, Daniel I Bromage, Ian J Wright, Anish Bhuva, Matthew J Lovell, Chris Plummer, Mark de Belder, Mark Dayer, Francis Murgatroyd","doi":"10.1136/openhrt-2025-003428","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The complication risk of procedures may be influenced by operator and institutional characteristics. Our aim was to assess whether supervising consultant seniority and operative volume, and hospital volume were associated with the risk of reintervention following complex device implantation.</p><p><strong>Methods: </strong>A nationwide population-based study was performed using the National Institute for Cardiovascular Outcomes Research registry including all patients receiving their first transvenous implantable cardioverter defibrillator or cardiac resynchronisation therapy (CRT) implant in England over 5 years (April 2014-March 2019). The primary endpoint was 1-year reintervention. We evaluated the association between reintervention and supervising consultant annualised complex device volume, supervising consultant seniority and hospital annualised complex device volume, using multilevel logistic regression.</p><p><strong>Results: </strong>47 630 implants were included. The 1-year reintervention rate was 6.1% (N=2916). There was no difference in reintervention risk with increasing supervising consultant volume (OR 0.89 Q4 vs Q1; 95% CI 0.76 to 1.05, p=0.17). When CRT-pacemakers/defibrillators implants were analysed separately (N=26 108), there was an association between operator volume and 1-year reintervention, but this was of borderline statistical significance and only evident in the highest compared with the lowest volume quartile of operators (adjusted OR 0.79 Q4 vs Q1; 95% CI 0.63 to 0.98, p=0.03). There was a non-linear relationship between reintervention risk and supervising consultant seniority, with the operators in the middle two quartiles of seniority having a lower risk (OR 0.87 Q2 vs Q1, p=0.02; OR 0.81 Q3 vs.Q1; p=0.003) while the most and least senior operators had a similar reintervention risk (OR 0.93 Q4 vs Q1, p=0.31). Hospital volume was not associated with 1-year reintervention.</p><p><strong>Conclusions: </strong>There is a U-shaped curve between operator seniority and reintervention risk for complex devices. Although there are several potential explanations, these data suggest that while newly qualified consultants may benefit from mentoring, all operators should continuously evaluate their outcomes and share them within their centre and more widely through the national audit.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 2","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12410664/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2025-003428","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The complication risk of procedures may be influenced by operator and institutional characteristics. Our aim was to assess whether supervising consultant seniority and operative volume, and hospital volume were associated with the risk of reintervention following complex device implantation.
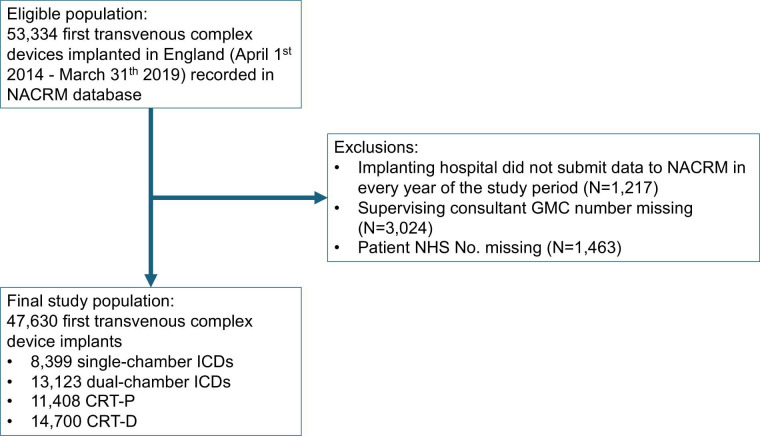
Methods: A nationwide population-based study was performed using the National Institute for Cardiovascular Outcomes Research registry including all patients receiving their first transvenous implantable cardioverter defibrillator or cardiac resynchronisation therapy (CRT) implant in England over 5 years (April 2014-March 2019). The primary endpoint was 1-year reintervention. We evaluated the association between reintervention and supervising consultant annualised complex device volume, supervising consultant seniority and hospital annualised complex device volume, using multilevel logistic regression.
Results: 47 630 implants were included. The 1-year reintervention rate was 6.1% (N=2916). There was no difference in reintervention risk with increasing supervising consultant volume (OR 0.89 Q4 vs Q1; 95% CI 0.76 to 1.05, p=0.17). When CRT-pacemakers/defibrillators implants were analysed separately (N=26 108), there was an association between operator volume and 1-year reintervention, but this was of borderline statistical significance and only evident in the highest compared with the lowest volume quartile of operators (adjusted OR 0.79 Q4 vs Q1; 95% CI 0.63 to 0.98, p=0.03). There was a non-linear relationship between reintervention risk and supervising consultant seniority, with the operators in the middle two quartiles of seniority having a lower risk (OR 0.87 Q2 vs Q1, p=0.02; OR 0.81 Q3 vs.Q1; p=0.003) while the most and least senior operators had a similar reintervention risk (OR 0.93 Q4 vs Q1, p=0.31). Hospital volume was not associated with 1-year reintervention.
Conclusions: There is a U-shaped curve between operator seniority and reintervention risk for complex devices. Although there are several potential explanations, these data suggest that while newly qualified consultants may benefit from mentoring, all operators should continuously evaluate their outcomes and share them within their centre and more widely through the national audit.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


