Kristina Sevcik, Claire Jackson, Shelly M Williams, Scott A Koepsell, Aleh Bobr
{"title":"Novel Red Blood Cell Exchange Parameters for Treatment of Transfusion-Dependent Thalassemia Based on Experience of Five Patients.","authors":"Kristina Sevcik, Claire Jackson, Shelly M Williams, Scott A Koepsell, Aleh Bobr","doi":"10.14740/jh2086","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Thalassemias are inherited red blood cell disorders characterized by defective globin production, resulting in microcytic hypochromic anemia. Severe variants lead to transfusion dependence and consequent iron overload, often despite chelation therapy. The role of automated red blood cell exchange (RBCX) for transfusion-dependent thalassemia (TDT) is unclear and previously there was no specific apheresis parameters specific for thalassemia defined. We present our experience with patients with TDT treated with RBCX using higher hematocrit parameters specifically tailored for this condition.</p><p><strong>Methods: </strong>Five patients with TDT underwent chronic RBCX in place of simple transfusion with the primary goal of stabilizing iron overload. Novel parameters were established to satisfy the Thalassemia International Federation goal pre-transfusion hemoglobin of 9.5 g/dL, while targeting a post-transfusion hematocrit of 37-38%.</p><p><strong>Results: </strong>RBCX was well tolerated with infrequent occurrences of vasovagal reactions, asymptomatic hypotension, citrate side effects, and vascular access issues. The transfusion interval increased from an average of 3 weeks with simple transfusions to 5 weeks with RBCX. Despite an increase in average blood utilization, serum ferritin levels remained stable.</p><p><strong>Conclusion: </strong>RBCX with higher hematocrit parameters can be performed safely and efficiently in TDT patients. To our knowledge, this is the first report of TDT-specific RBCX parameters. Though blood utilization is higher with RBCX, it offers longer intervals between transfusions and has no increase in iron overload, improving quality of life for patients.</p>","PeriodicalId":15964,"journal":{"name":"Journal of hematology","volume":"14 4","pages":"210-213"},"PeriodicalIF":1.3000,"publicationDate":"2025-07-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404126/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jh2086","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Thalassemias are inherited red blood cell disorders characterized by defective globin production, resulting in microcytic hypochromic anemia. Severe variants lead to transfusion dependence and consequent iron overload, often despite chelation therapy. The role of automated red blood cell exchange (RBCX) for transfusion-dependent thalassemia (TDT) is unclear and previously there was no specific apheresis parameters specific for thalassemia defined. We present our experience with patients with TDT treated with RBCX using higher hematocrit parameters specifically tailored for this condition.
Methods: Five patients with TDT underwent chronic RBCX in place of simple transfusion with the primary goal of stabilizing iron overload. Novel parameters were established to satisfy the Thalassemia International Federation goal pre-transfusion hemoglobin of 9.5 g/dL, while targeting a post-transfusion hematocrit of 37-38%.
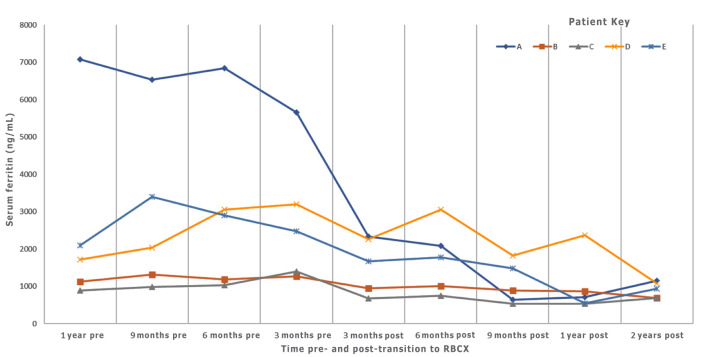
Results: RBCX was well tolerated with infrequent occurrences of vasovagal reactions, asymptomatic hypotension, citrate side effects, and vascular access issues. The transfusion interval increased from an average of 3 weeks with simple transfusions to 5 weeks with RBCX. Despite an increase in average blood utilization, serum ferritin levels remained stable.
Conclusion: RBCX with higher hematocrit parameters can be performed safely and efficiently in TDT patients. To our knowledge, this is the first report of TDT-specific RBCX parameters. Though blood utilization is higher with RBCX, it offers longer intervals between transfusions and has no increase in iron overload, improving quality of life for patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


