Association of patient, physician and visit characteristics with inappropriate antibiotic prescribing in Japanese primary care: a cross-sectional study.
Atsushi Miyawaki, Joseph B Ladines-Lim, Daichi Sato, Kei Kitajima, Jeffrey A Linder, Michael A Fischer, Kao-Ping Chua, Yusuke Tsugawa
{"title":"Association of patient, physician and visit characteristics with inappropriate antibiotic prescribing in Japanese primary care: a cross-sectional study.","authors":"Atsushi Miyawaki, Joseph B Ladines-Lim, Daichi Sato, Kei Kitajima, Jeffrey A Linder, Michael A Fischer, Kao-Ping Chua, Yusuke Tsugawa","doi":"10.1136/bmjph-2024-002364","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong></p><p><strong>Objective: </strong>To assess the prevalence and associated factors of inappropriate antibiotic prescribing in Japanese primary care.</p><p><strong>Methods: </strong>This cross-sectional study analysed all antibiotic prescriptions written between 1 October 2022 and 30 September 2023, using an electronic health record database of primary care clinics across Japan. Using a previously developed classification algorithm, we determined whether diagnosis codes occurring on or during the 3 days before the antibiotic prescribing date 'always', 'sometimes' or 'never' justified antibiotic use. We classified antibiotic prescriptions into one of four mutually exclusive categories: 'appropriate' (associated with ≥1 'always' code), 'potentially appropriate' (associated with ≥1 'sometimes' code but no 'always' codes), 'inappropriate' (associated only with 'never' codes) and 'not associated with a recent diagnosis'. A linear probability model examined patient, physician and visit characteristics associated with inappropriate antibiotic prescribing among solo practice clinics.</p><p><strong>Results: </strong>Analyses included 2 058 021 outpatient antibiotic prescriptions to 1 267 708 patients at 2809 clinics. Among these prescriptions, 176 181 (8.6%) were appropriate, 1 238 549 (60.2%) were potentially appropriate, 348 949 (17.0%) were inappropriate and 294 342 (14.3%) were not associated with a recent diagnosis. Among solo practice clinics, inappropriate prescribing was more likely to patients aged <18 versus ≥65 years (+2.6%; 95% CI +0.3% to +4.9%) or with Charlson Comorbidity Index score ≥2 vs 0 (+2.0%; 95% CI +0.6% to +3.4%), for physicians aged ≥65 versus <45 years (+7.3%; 95% CI +3.6% to +11.0%), for physicians in the highest tertile of antibiotic prescribing volume (+4.9%; 95% CI +3.0% to +6.8%), during telehealth visits (+3.9% vs office visits; 95% CI +0.02% to +7.7%) and during regular hours care versus after hours care (+2.1%; 95% CI +0.7% to +3.5%). These findings were qualitatively unchanged when including both solo and group practice clinics.</p><p><strong>Conclusions: </strong>Targeting younger patients, patients with comorbidities, older physicians, physicians with high antibiotic prescribing, telehealth visits and regular hours care may further increase stewardship effectiveness.</p>","PeriodicalId":101362,"journal":{"name":"BMJ public health","volume":"3 2","pages":"e002364"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366620/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ public health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjph-2024-002364","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Abstract:
Objective: To assess the prevalence and associated factors of inappropriate antibiotic prescribing in Japanese primary care.
Methods: This cross-sectional study analysed all antibiotic prescriptions written between 1 October 2022 and 30 September 2023, using an electronic health record database of primary care clinics across Japan. Using a previously developed classification algorithm, we determined whether diagnosis codes occurring on or during the 3 days before the antibiotic prescribing date 'always', 'sometimes' or 'never' justified antibiotic use. We classified antibiotic prescriptions into one of four mutually exclusive categories: 'appropriate' (associated with ≥1 'always' code), 'potentially appropriate' (associated with ≥1 'sometimes' code but no 'always' codes), 'inappropriate' (associated only with 'never' codes) and 'not associated with a recent diagnosis'. A linear probability model examined patient, physician and visit characteristics associated with inappropriate antibiotic prescribing among solo practice clinics.
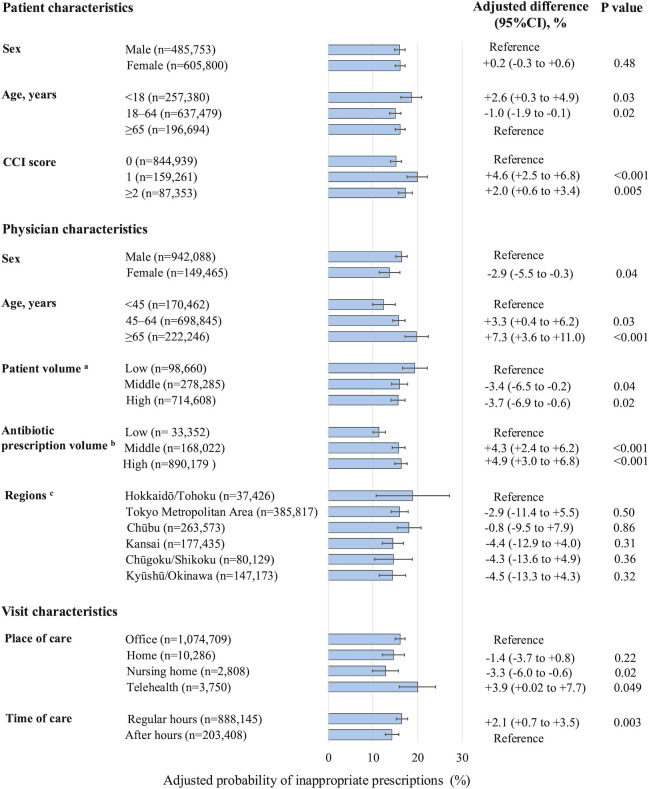
Results: Analyses included 2 058 021 outpatient antibiotic prescriptions to 1 267 708 patients at 2809 clinics. Among these prescriptions, 176 181 (8.6%) were appropriate, 1 238 549 (60.2%) were potentially appropriate, 348 949 (17.0%) were inappropriate and 294 342 (14.3%) were not associated with a recent diagnosis. Among solo practice clinics, inappropriate prescribing was more likely to patients aged <18 versus ≥65 years (+2.6%; 95% CI +0.3% to +4.9%) or with Charlson Comorbidity Index score ≥2 vs 0 (+2.0%; 95% CI +0.6% to +3.4%), for physicians aged ≥65 versus <45 years (+7.3%; 95% CI +3.6% to +11.0%), for physicians in the highest tertile of antibiotic prescribing volume (+4.9%; 95% CI +3.0% to +6.8%), during telehealth visits (+3.9% vs office visits; 95% CI +0.02% to +7.7%) and during regular hours care versus after hours care (+2.1%; 95% CI +0.7% to +3.5%). These findings were qualitatively unchanged when including both solo and group practice clinics.
Conclusions: Targeting younger patients, patients with comorbidities, older physicians, physicians with high antibiotic prescribing, telehealth visits and regular hours care may further increase stewardship effectiveness.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


