Siddharth Srinivasan, Anna Craig-McQuaide, Mustafa Elsheikh, Dhanwanth Chigurupati, Rishikesh Ravindran, Shivani Rajkumar, Saif Khan, Christopher Pollard, Calan Mathieson
{"title":"Cocaine-Induced Midline Destructive Lesions-A Harbinger of Meningitis and Hydrocephalus.","authors":"Siddharth Srinivasan, Anna Craig-McQuaide, Mustafa Elsheikh, Dhanwanth Chigurupati, Rishikesh Ravindran, Shivani Rajkumar, Saif Khan, Christopher Pollard, Calan Mathieson","doi":"10.1055/s-0045-1808235","DOIUrl":null,"url":null,"abstract":"<p><p>Cocaine is among the most commonly used recreational drugs in Scotland, contributing to significant socioeconomic and severe health challenges. The prevalence of cocaine-induced midline destructive lesions (CIMDL) is rising due to increased cocaine insufflation. Here, we report a case of a patient who developed acute hydrocephalus and meningitis as complications of CIMDL due to long-term cocaine abuse. A 39-year-old woman with a history of chronic nasal cocaine abuse presented with fever, malaise, and gait imbalance. On arrival at accident and emergency department, she had altered sensorium, Glasgow coma scale (GCS) of 10, and left-sided hemiparesis, requiring emergency intubation. Imaging revealed acute hydrocephalus and brain edema. She underwent an emergency external ventricular drain (EVD) to temporize her raised intracranial pressure. Her constellation of problems and biochemical parameters directed toward a diagnosis of acute bacterial meningitis. Her blood cultures grew methicillin-sensitive <i>Staphylococcus aureus</i> , and she was started on broad-spectrum antibiotics. Her computed tomography scans showed air in the sphenoid sinus, clival erosion, and partial erosion of the anterior arch of C1, consistent with CIMDL. She developed posterior circulation ischemic strokes, which were attributed to her endocarditis and tricuspid valve vegetations that were detected on her transthoracic echocardiogram. Eventually, she underwent a ventriculoperitoneal shunt for permanent cerebrospinal fluid diversion. Neurologically, she was E4V5M6 with residual left hemiparesis at the time of discharge. She is on aggressive rehabilitation under the care of oral maxillofacial surgery, otorhinolaryngology, and a skull base team for her CIMDL. This case highlights the importance of multidisciplinary care and support in managing such cases, especially aiming to prevent the recurrence of infection leading to significant morbidity or even mortality.</p>","PeriodicalId":94300,"journal":{"name":"Asian journal of neurosurgery","volume":"20 3","pages":"627-630"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12370344/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian journal of neurosurgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0045-1808235","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
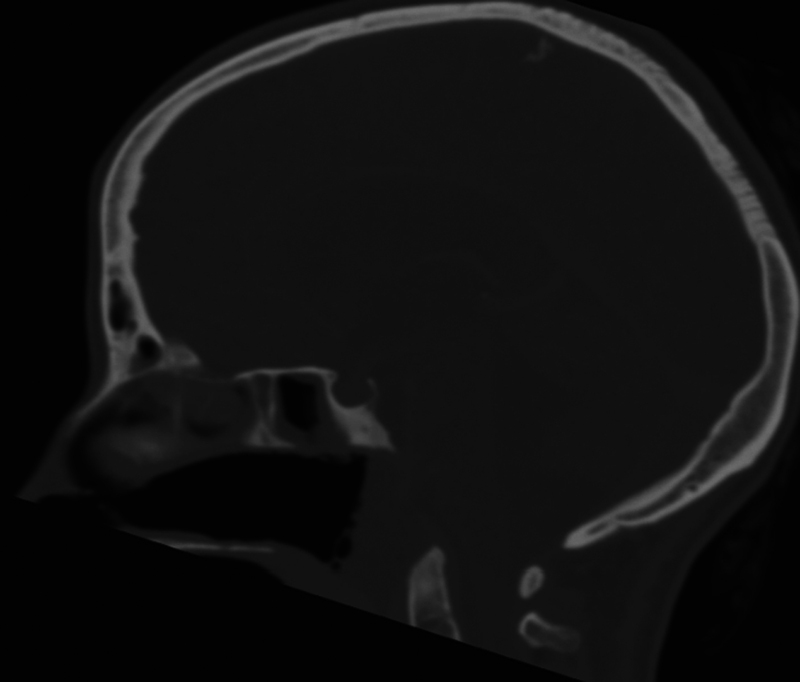
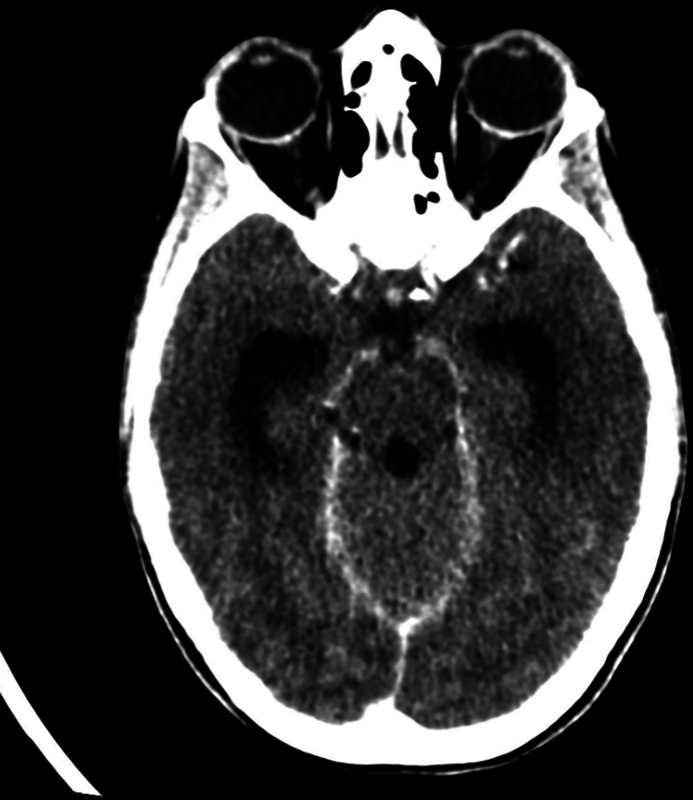
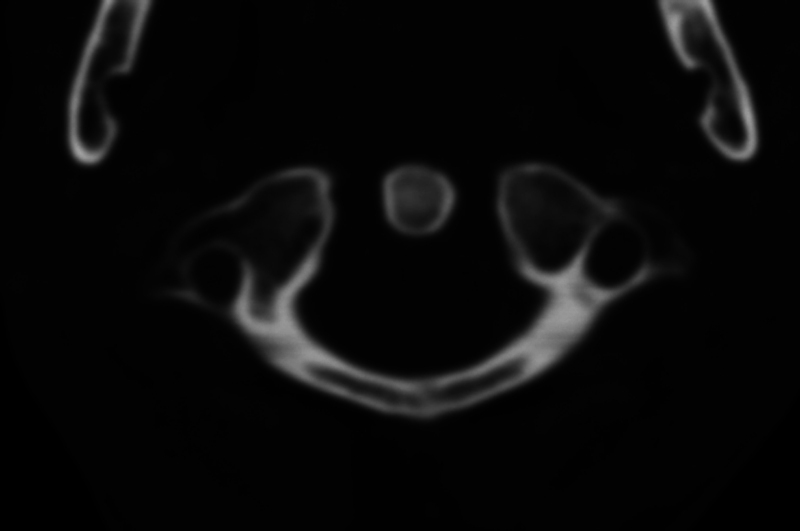
Cocaine is among the most commonly used recreational drugs in Scotland, contributing to significant socioeconomic and severe health challenges. The prevalence of cocaine-induced midline destructive lesions (CIMDL) is rising due to increased cocaine insufflation. Here, we report a case of a patient who developed acute hydrocephalus and meningitis as complications of CIMDL due to long-term cocaine abuse. A 39-year-old woman with a history of chronic nasal cocaine abuse presented with fever, malaise, and gait imbalance. On arrival at accident and emergency department, she had altered sensorium, Glasgow coma scale (GCS) of 10, and left-sided hemiparesis, requiring emergency intubation. Imaging revealed acute hydrocephalus and brain edema. She underwent an emergency external ventricular drain (EVD) to temporize her raised intracranial pressure. Her constellation of problems and biochemical parameters directed toward a diagnosis of acute bacterial meningitis. Her blood cultures grew methicillin-sensitive Staphylococcus aureus , and she was started on broad-spectrum antibiotics. Her computed tomography scans showed air in the sphenoid sinus, clival erosion, and partial erosion of the anterior arch of C1, consistent with CIMDL. She developed posterior circulation ischemic strokes, which were attributed to her endocarditis and tricuspid valve vegetations that were detected on her transthoracic echocardiogram. Eventually, she underwent a ventriculoperitoneal shunt for permanent cerebrospinal fluid diversion. Neurologically, she was E4V5M6 with residual left hemiparesis at the time of discharge. She is on aggressive rehabilitation under the care of oral maxillofacial surgery, otorhinolaryngology, and a skull base team for her CIMDL. This case highlights the importance of multidisciplinary care and support in managing such cases, especially aiming to prevent the recurrence of infection leading to significant morbidity or even mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


