Comparative Analysis of Bite Force after Cranioplasty with and without Temporalis Dissection in Large Skull Defects Caused by Decompressive Craniectomy.
Soumya Deepta Nandi, Raja K Kutty, Jyothish Laila Sivanandapanicker, Sunilkumar Balakrishnan Sreemathyamma, Raj S Chandran, Rosebist Pathrose Kamalabai, Libu Gnanaseelan Kanakamma, Rajmohan Bhanu Prabhakar, Sureshkumar Kunjuni Leela, Anilkumar Peethambaran
{"title":"Comparative Analysis of Bite Force after Cranioplasty with and without Temporalis Dissection in Large Skull Defects Caused by Decompressive Craniectomy.","authors":"Soumya Deepta Nandi, Raja K Kutty, Jyothish Laila Sivanandapanicker, Sunilkumar Balakrishnan Sreemathyamma, Raj S Chandran, Rosebist Pathrose Kamalabai, Libu Gnanaseelan Kanakamma, Rajmohan Bhanu Prabhakar, Sureshkumar Kunjuni Leela, Anilkumar Peethambaran","doi":"10.1055/s-0045-1809047","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cranioplasty involves repairing the skull defect using an autologous bone flap or synthetic molds. The temporalis muscle, detached during decompressive craniectomy (DC), may be reattached to the bone flap for better cosmetic reconstruction. Along with the masseter and pterygoid muscles, the temporalis muscle significantly contributes to the human bite force. In this study, we analyze patients' bite force in which the temporalis muscle was either dissected and reattached or left undisturbed during cranioplasty.</p><p><strong>Materials and methods: </strong>All patients who previously underwent DC for traumatic brain injury or stroke were grouped into two, depending on the method of cranioplasty. In group 1, patients underwent temporalis muscle dissection and reattachment to the bone flap or prosthesis. In group 2, the temporalis muscle was left undisturbed. The bite force of the subjects was measured bilaterally in both groups by a gnathodynamometer before cranioplasty and 3 months after the surgery. We compared the difference in bite force of the subjects individually on both sides, preoperatively and postoperatively, as well as between the groups.</p><p><strong>Results: </strong>This study included 36 patients over 18 years of age, with 18 patients in each group. Preoperatively, the bite force of all the subjects was decreased on the side of the DC compared with the normal side. After cranioplasty, the bite force significantly improved compared with preoperative values in both groups.</p><p><strong>Conclusion: </strong>Temporalis dissection can be safely done during cranioplasty. There is improvement in bite force after cranioplasty with or without temporalis dissection.</p>","PeriodicalId":94300,"journal":{"name":"Asian journal of neurosurgery","volume":"20 3","pages":"542-548"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12370351/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian journal of neurosurgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0045-1809047","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
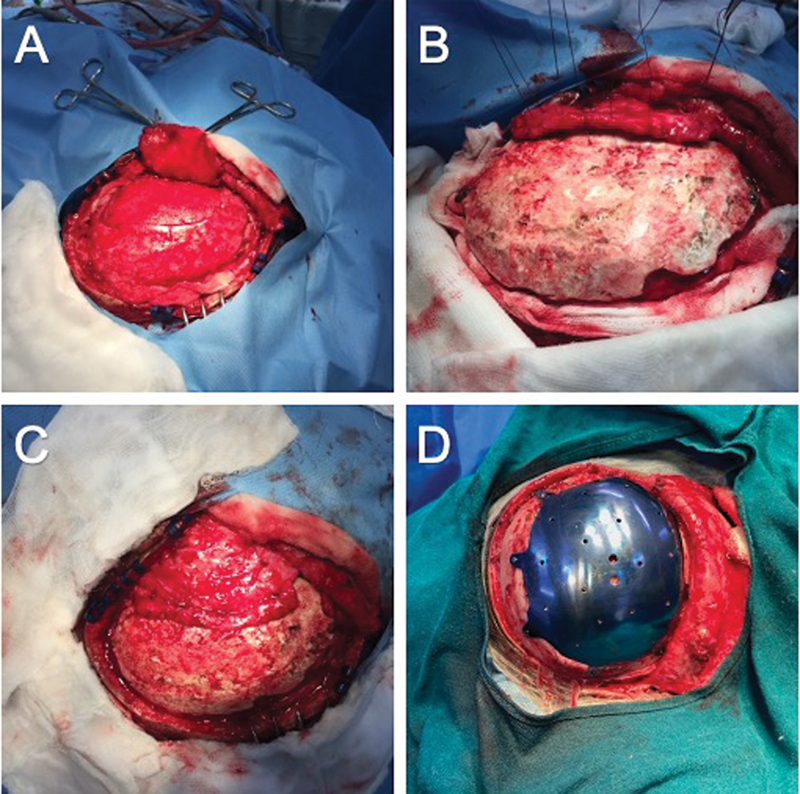
Introduction: Cranioplasty involves repairing the skull defect using an autologous bone flap or synthetic molds. The temporalis muscle, detached during decompressive craniectomy (DC), may be reattached to the bone flap for better cosmetic reconstruction. Along with the masseter and pterygoid muscles, the temporalis muscle significantly contributes to the human bite force. In this study, we analyze patients' bite force in which the temporalis muscle was either dissected and reattached or left undisturbed during cranioplasty.
Materials and methods: All patients who previously underwent DC for traumatic brain injury or stroke were grouped into two, depending on the method of cranioplasty. In group 1, patients underwent temporalis muscle dissection and reattachment to the bone flap or prosthesis. In group 2, the temporalis muscle was left undisturbed. The bite force of the subjects was measured bilaterally in both groups by a gnathodynamometer before cranioplasty and 3 months after the surgery. We compared the difference in bite force of the subjects individually on both sides, preoperatively and postoperatively, as well as between the groups.
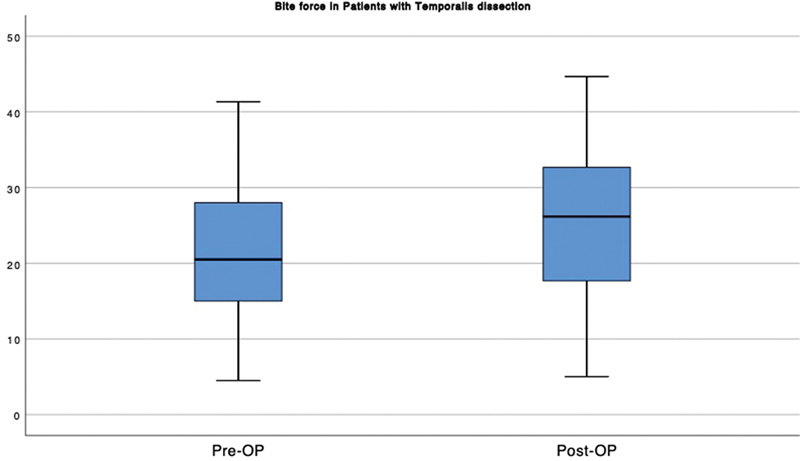
Results: This study included 36 patients over 18 years of age, with 18 patients in each group. Preoperatively, the bite force of all the subjects was decreased on the side of the DC compared with the normal side. After cranioplasty, the bite force significantly improved compared with preoperative values in both groups.
Conclusion: Temporalis dissection can be safely done during cranioplasty. There is improvement in bite force after cranioplasty with or without temporalis dissection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


