Delayed presentation of esophageal perforation from anterior cervical discectomy and fusion hardware failure in a patient presenting with non-ST-elevation myocardial infarction: An illustrative technical note.
{"title":"Delayed presentation of esophageal perforation from anterior cervical discectomy and fusion hardware failure in a patient presenting with non-ST-elevation myocardial infarction: An illustrative technical note.","authors":"Tyler Nicole Lackland, Mayur Patel, Kathleen Suzann Botterbush, Joseph J Platz, Mauricio J Avila","doi":"10.25259/SNI_242_2025","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A 69-year-old male, who underwent a C5-T1 ACDF 5-years prior to arrival, presented with a ventral pharyngeal abscess and esophageal perforation warranting major gastro-esophageal surgery and instrumentation removal.</p><p><strong>Methods: </strong>The case of a patient who underwent a C5-T1 ACDF five years ago was reviewed. A review of past reports of cases of patients who experienced esophageal erosion or perforation following ACDF was conducted.</p><p><strong>Results: </strong>At the age of 69, the patient acutely developed disorientation/agitation and urinary/fecal incontinence. Lab studies showed leukocytosis, an elevated creatine phosphokinase (CPK), and lactic acidosis, while the EKG confirmed a non-ST-elevation myocardial infarction (NSTEMI) with increased troponins. An esophagram revealed esophageal perforation, and a prevertebral C5-C6 abscess, and neck/thoracic CT studies documented 8-9 mm anterior displacement of the right inferior C7 screw with extravasation extending inferiorly into the mediastinum. Surgery consisted of an esophagogastroduodenoscopy, gastric/jejunal tube placement, left neck exploration, and dissection of the esophagus off the anterior instrumentation that was subsequently removed. Despite emergent surgical intervention, the patient expired 5 days postoperatively.</p><p><strong>Conclusion: </strong>Neurosurgical follow-up is warranted in ACDF patients who newly present with findings indicative of with anterior retropharyngeal abscess or esophageal perforation.</p>","PeriodicalId":94217,"journal":{"name":"Surgical neurology international","volume":"16 ","pages":"299"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361707/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical neurology international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/SNI_242_2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A 69-year-old male, who underwent a C5-T1 ACDF 5-years prior to arrival, presented with a ventral pharyngeal abscess and esophageal perforation warranting major gastro-esophageal surgery and instrumentation removal.
Methods: The case of a patient who underwent a C5-T1 ACDF five years ago was reviewed. A review of past reports of cases of patients who experienced esophageal erosion or perforation following ACDF was conducted.
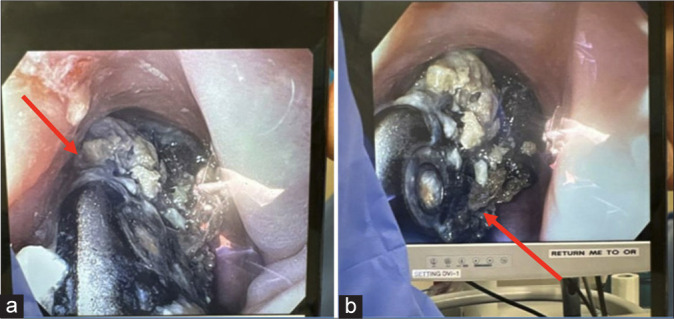
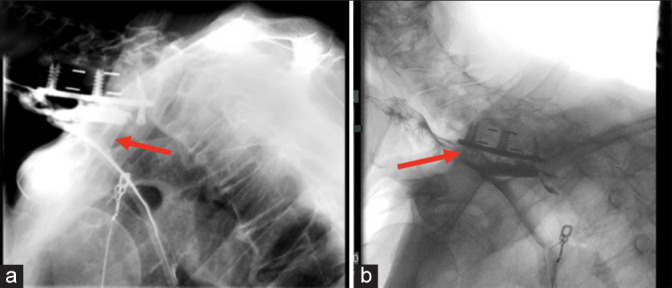
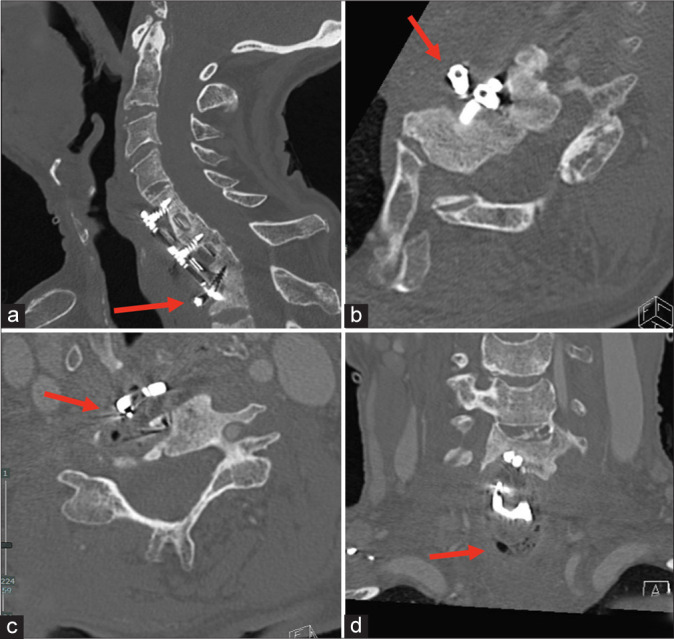
Results: At the age of 69, the patient acutely developed disorientation/agitation and urinary/fecal incontinence. Lab studies showed leukocytosis, an elevated creatine phosphokinase (CPK), and lactic acidosis, while the EKG confirmed a non-ST-elevation myocardial infarction (NSTEMI) with increased troponins. An esophagram revealed esophageal perforation, and a prevertebral C5-C6 abscess, and neck/thoracic CT studies documented 8-9 mm anterior displacement of the right inferior C7 screw with extravasation extending inferiorly into the mediastinum. Surgery consisted of an esophagogastroduodenoscopy, gastric/jejunal tube placement, left neck exploration, and dissection of the esophagus off the anterior instrumentation that was subsequently removed. Despite emergent surgical intervention, the patient expired 5 days postoperatively.
Conclusion: Neurosurgical follow-up is warranted in ACDF patients who newly present with findings indicative of with anterior retropharyngeal abscess or esophageal perforation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


