{"title":"Contrecoup raccoon sign following minor posterior head injury without visible injury: Diagnostic challenge in an asymptomatic older adult man.","authors":"Shintaro Tsuboguchi, Kouichirou Okamoto, Susumu Tokiguchi","doi":"10.25259/SNI_229_2025","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Traumatic raccoon sign (periorbital ecchymosis) typically results from facial or severe head trauma involving anterior skull base fractures. In contrast, contrecoup raccoon signs arising from minor posterior head injuries are extremely rare, particularly in older adults. In addition, spontaneous, nontraumatic raccoon signs may be associated with focal or systemic conditions, including malignancies, necessitating extensive diagnostic evaluation. Distinguishing between traumatic and nontraumatic causes is crucial in older patients presenting with raccoon sign following minor head trauma, especially when neurological deficits and visible external injuries are absent.</p><p><strong>Case description: </strong>An 85-year-old male with a 30-year history of insulin-treated type 2 diabetes presented with raccoon sign one morning, without additional symptoms. A comprehensive physical examination, including a detailed head assessment, revealed no abnormalities. However, computed tomography (CT) imaging identified a minor subarachnoid hemorrhage, and high-resolution CT imaging (1-mm bone slice thickness) detected a thin orbital roof fracture, confirming a traumatic contrecoup injury. This finding rendered the differential diagnosis for nontraumatic causes irrelevant. The patient's longstanding diabetes was considered a relevant factor in the development of the raccoon sign.</p><p><strong>Conclusion: </strong>In older adult patients presenting with raccoon sign but lacking overt symptoms, obtaining a thorough history of head trauma and diabetes is essential, even in cases of minor injury without visible external signs. High-resolution thin-slice bone CT imaging is vital for detecting subtle orbital roof fractures, which may otherwise go unnoticed. Early identification facilitates accurate diagnosis and prevents unnecessary evaluations for nontraumatic causes.</p>","PeriodicalId":94217,"journal":{"name":"Surgical neurology international","volume":"16 ","pages":"286"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361661/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical neurology international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/SNI_229_2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
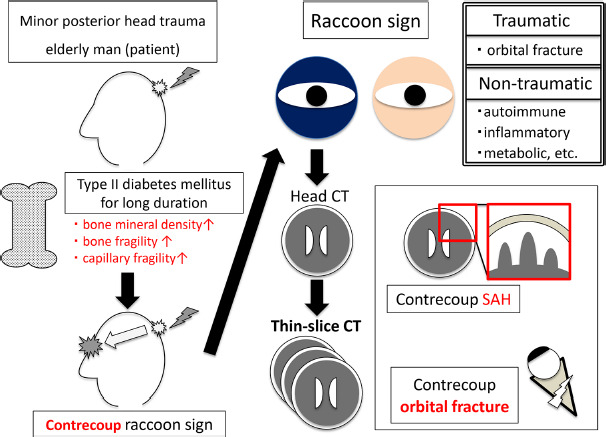
Background: Traumatic raccoon sign (periorbital ecchymosis) typically results from facial or severe head trauma involving anterior skull base fractures. In contrast, contrecoup raccoon signs arising from minor posterior head injuries are extremely rare, particularly in older adults. In addition, spontaneous, nontraumatic raccoon signs may be associated with focal or systemic conditions, including malignancies, necessitating extensive diagnostic evaluation. Distinguishing between traumatic and nontraumatic causes is crucial in older patients presenting with raccoon sign following minor head trauma, especially when neurological deficits and visible external injuries are absent.
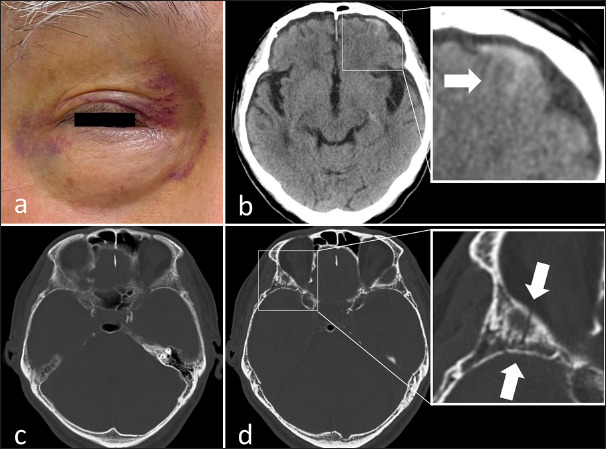
Case description: An 85-year-old male with a 30-year history of insulin-treated type 2 diabetes presented with raccoon sign one morning, without additional symptoms. A comprehensive physical examination, including a detailed head assessment, revealed no abnormalities. However, computed tomography (CT) imaging identified a minor subarachnoid hemorrhage, and high-resolution CT imaging (1-mm bone slice thickness) detected a thin orbital roof fracture, confirming a traumatic contrecoup injury. This finding rendered the differential diagnosis for nontraumatic causes irrelevant. The patient's longstanding diabetes was considered a relevant factor in the development of the raccoon sign.
Conclusion: In older adult patients presenting with raccoon sign but lacking overt symptoms, obtaining a thorough history of head trauma and diabetes is essential, even in cases of minor injury without visible external signs. High-resolution thin-slice bone CT imaging is vital for detecting subtle orbital roof fractures, which may otherwise go unnoticed. Early identification facilitates accurate diagnosis and prevents unnecessary evaluations for nontraumatic causes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


