Updated review of cervical white cord syndrome (WCS)/reperfusion injury (RI); A "diagnosis of inclusion" requiring magnetic resonance (MR) confirmation, not just a "clinical diagnosis".
{"title":"Updated review of cervical white cord syndrome (WCS)/reperfusion injury (RI); A \"diagnosis of inclusion\" requiring magnetic resonance (MR) confirmation, not just a \"clinical diagnosis\".","authors":"Nancy E Epstein, Marc A Agulnick","doi":"10.25259/SNI_603_2025","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Cervical White Cord Syndrome (WCS)/Reperfusion Injury (RI) rarely causes new major postoperative neurological deficits, and is attributed to the rapid surgical decompression of a chronically compressed/ischemic cord. Never a diagnosis based on \"clinical judgment\" alone, the WCS/RI is a <i>diagnosis of inclusion</i> that requires emergent postoperative MR confirmation of the classical \"white cord\" (i.e., high intrinsic T2W MR cord signal reflecting edema/swelling).</p><p><strong>Methods: </strong>Most frequently, postoperative MR studies in newly paretic/injured patients following cervical operations will show evidence of direct intraoperative (\"iatrogenic\") spinal cord injury. Less frequently, findings may include new non-operative vs. operative pathology (i.e., hematomas/hematomyelia, graft extrusions/malpositioning, new/residual/recurrent disc/stenosis/Ossification of the Posterior Longitudinal Ligament (OPLL), and other pathology).</p><p><strong>Results: </strong>WCS/RI after cervical spine surgery is extremely rare, being reported in only 17 cases as of 2020, and cannot be diagnosed based on \"clinical judgment\" alone; rather, it requires a STAT corroborate postoperative MR to demonstrate the classical \"white cord\". However, most likely postoperative MR studies document \"iatrogenic\" cord injuries, and less likely show new non-surgical and/or new surgical compressive pathology warranting reoperations to remediate the extent/severity of neurological injuries.</p><p><strong>Conclusion: </strong>The postoperative diagnosis of WCS/RI should never be established based on \"clinical judgment alone\". Rather, WCS/RI is a <i>diagnosis of inclusion</i> that requires STAT postoperative MR documentation of the classical swollen/edematous \"white cord\".</p>","PeriodicalId":94217,"journal":{"name":"Surgical neurology international","volume":"16 ","pages":"279"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361648/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical neurology international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/SNI_603_2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
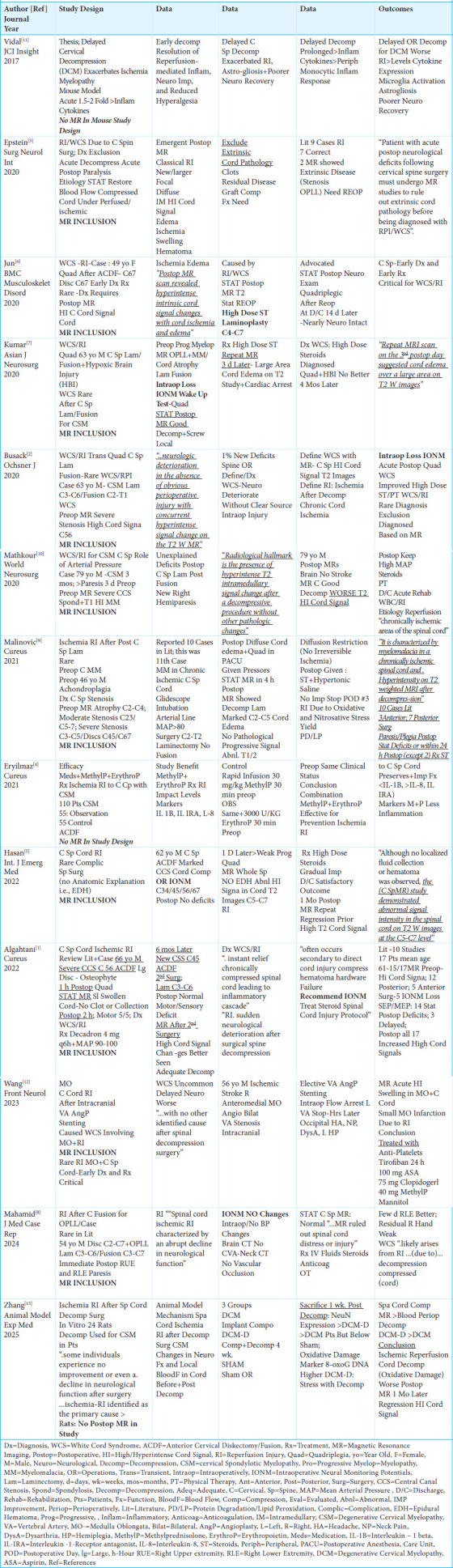
Background: The Cervical White Cord Syndrome (WCS)/Reperfusion Injury (RI) rarely causes new major postoperative neurological deficits, and is attributed to the rapid surgical decompression of a chronically compressed/ischemic cord. Never a diagnosis based on "clinical judgment" alone, the WCS/RI is a diagnosis of inclusion that requires emergent postoperative MR confirmation of the classical "white cord" (i.e., high intrinsic T2W MR cord signal reflecting edema/swelling).
Methods: Most frequently, postoperative MR studies in newly paretic/injured patients following cervical operations will show evidence of direct intraoperative ("iatrogenic") spinal cord injury. Less frequently, findings may include new non-operative vs. operative pathology (i.e., hematomas/hematomyelia, graft extrusions/malpositioning, new/residual/recurrent disc/stenosis/Ossification of the Posterior Longitudinal Ligament (OPLL), and other pathology).
Results: WCS/RI after cervical spine surgery is extremely rare, being reported in only 17 cases as of 2020, and cannot be diagnosed based on "clinical judgment" alone; rather, it requires a STAT corroborate postoperative MR to demonstrate the classical "white cord". However, most likely postoperative MR studies document "iatrogenic" cord injuries, and less likely show new non-surgical and/or new surgical compressive pathology warranting reoperations to remediate the extent/severity of neurological injuries.
Conclusion: The postoperative diagnosis of WCS/RI should never be established based on "clinical judgment alone". Rather, WCS/RI is a diagnosis of inclusion that requires STAT postoperative MR documentation of the classical swollen/edematous "white cord".


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


