{"title":"Low-degree rotation and chin-up head position for resection of glioblastomas extending into the medial part of the temporal lobe.","authors":"Hirotaka Inoue, Jun-Ichiro Kuroda, Tadashi Hamasaki, Akitake Mukasa","doi":"10.25259/SNI_307_2025","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The anterior choroidal artery and lateral posterior choroidal artery are vital structures preserved during the microsurgical treatment of glioblastomas in the temporal lobe. Nevertheless, few studies have examined the appropriate head position for identifying the choroidal arteries in resecting such glioblastomas. In general, a 45°-90° rotation to the opposite side of the lesion is commonly used; however, we have utilized a low-degree rotation (LDR) and chin-up (CU) head position.</p><p><strong>Methods: </strong>The LDR is 30-40° rotation to the opposite side of the lesion. The CU is the angle at which the line connecting the nasion and inion is tilted approximately 30° from the vertical. We retrospectively assessed six consecutive patients with glioblastomas extending into the medial part of the temporal lobe that was resected using the LDR and CU.</p><p><strong>Results: </strong>None of our six patients had an infarction in the area of the choroidal artery or any surgery-related adverse symptoms. The choroidal arteries and hippocampus were not at the deepest point of the resection cavity in the LDR and CU; therefore, these structures were identified during the early phase of surgery.</p><p><strong>Conclusion: </strong>We suggest that the LDR and CU are suitable for resecting glioblastomas extending into the medial part of the temporal lobe.</p>","PeriodicalId":94217,"journal":{"name":"Surgical neurology international","volume":"16 ","pages":"285"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361703/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical neurology international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/SNI_307_2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The anterior choroidal artery and lateral posterior choroidal artery are vital structures preserved during the microsurgical treatment of glioblastomas in the temporal lobe. Nevertheless, few studies have examined the appropriate head position for identifying the choroidal arteries in resecting such glioblastomas. In general, a 45°-90° rotation to the opposite side of the lesion is commonly used; however, we have utilized a low-degree rotation (LDR) and chin-up (CU) head position.
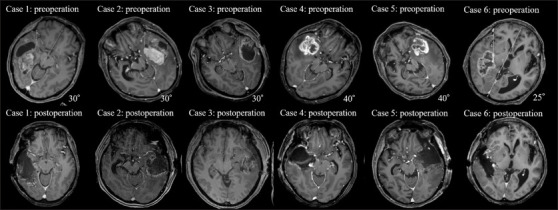
Methods: The LDR is 30-40° rotation to the opposite side of the lesion. The CU is the angle at which the line connecting the nasion and inion is tilted approximately 30° from the vertical. We retrospectively assessed six consecutive patients with glioblastomas extending into the medial part of the temporal lobe that was resected using the LDR and CU.
Results: None of our six patients had an infarction in the area of the choroidal artery or any surgery-related adverse symptoms. The choroidal arteries and hippocampus were not at the deepest point of the resection cavity in the LDR and CU; therefore, these structures were identified during the early phase of surgery.
Conclusion: We suggest that the LDR and CU are suitable for resecting glioblastomas extending into the medial part of the temporal lobe.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


