{"title":"Perioperative antihypertensive medications and effects on functional decline and mortality in non-cardiac surgery.","authors":"Rena Suzukawa, Shintaro Mandai, Yuta Nakano, Shunsuke Inaba, Hisazumi Matsuki, Yutaro Mori, Fumiaki Ando, Takayasu Mori, Koichiro Susa, Soichiro Iimori, Shotaro Naito, Eisei Sohara, Tatemitsu Rai, Kiyohide Fushimi, Shinichi Uchida","doi":"10.1093/ehjopen/oeaf096","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The association between perioperative antihypertensive drugs and mortality as well as physical function in non-cardiac surgeries remains unclear. We aimed to clarify the association between six antihypertensive classes and postoperative outcomes.</p><p><strong>Methods and results: </strong>This observational cohort study involved adults undergoing non-cardiac surgeries between 2014 and 2019 using an administrative claims database. We recruited 408 810 patients who continuously used any class of antihypertensive medication both pre- and postoperatively and 2 190 064 non-continuous users aged ≥50 years who underwent five different types of non-cardiac surgeries. The risk for overall death or functional decline, defined as a ≥20% decrease in the Barthel Index score during hospitalization, was determined using multivariable logistic regression models. All-cause deaths or functional decline occurred in 4228 (1.0%) users and 17 978 (0.8%) non-users or 20 625 (5.0%) users and 66 218 (3.0%) non-users, respectively. Among single-class users, angiotensin-converting enzyme inhibitors (ACEis) or angiotensin II receptor blockers (ARBs) showed a multivariable odds ratio (OR) of 0.74 [95% confidence interval (CI) 0.62-0.89 vs. thiazide/thiazide-like diuretics (TH)] for the composite of mortality and functional decline. Among recipients of two medication classes, calcium receptor blockers (CCBs)/ACEi or ARB usage was associated with the lowest risk for composite outcome (OR, 0.86; 95% CI, 0.81-0.91 vs. TH/CCBs). The combinations of the ≥3 classes, including TH/CCB/ACEi or ARB, displayed the lowest odds for the composite outcome. In orthopaedic surgery and gastrointestinal resection, ACEis or ARBs were associated with better survival and physical function.</p><p><strong>Conclusion: </strong>Perioperative use of ACEis or ARBs is associated with favourable outcomes in non-cardiac surgeries.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 4","pages":"oeaf096"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12393147/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf096","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
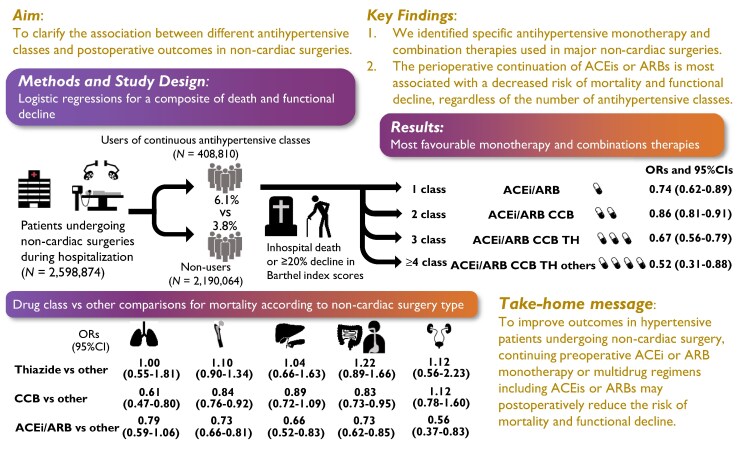
Aims: The association between perioperative antihypertensive drugs and mortality as well as physical function in non-cardiac surgeries remains unclear. We aimed to clarify the association between six antihypertensive classes and postoperative outcomes.
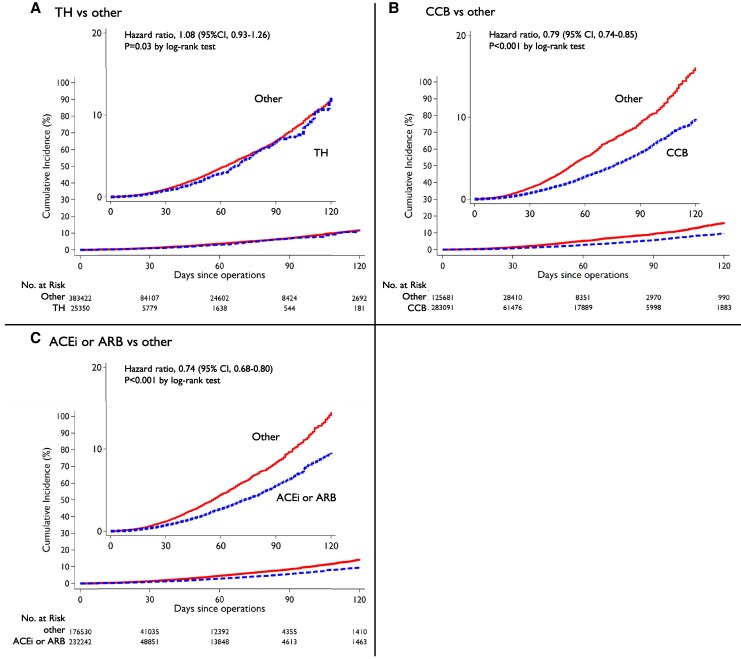
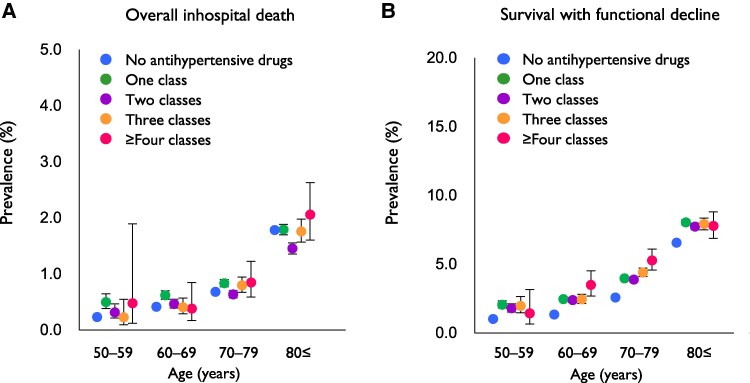
Methods and results: This observational cohort study involved adults undergoing non-cardiac surgeries between 2014 and 2019 using an administrative claims database. We recruited 408 810 patients who continuously used any class of antihypertensive medication both pre- and postoperatively and 2 190 064 non-continuous users aged ≥50 years who underwent five different types of non-cardiac surgeries. The risk for overall death or functional decline, defined as a ≥20% decrease in the Barthel Index score during hospitalization, was determined using multivariable logistic regression models. All-cause deaths or functional decline occurred in 4228 (1.0%) users and 17 978 (0.8%) non-users or 20 625 (5.0%) users and 66 218 (3.0%) non-users, respectively. Among single-class users, angiotensin-converting enzyme inhibitors (ACEis) or angiotensin II receptor blockers (ARBs) showed a multivariable odds ratio (OR) of 0.74 [95% confidence interval (CI) 0.62-0.89 vs. thiazide/thiazide-like diuretics (TH)] for the composite of mortality and functional decline. Among recipients of two medication classes, calcium receptor blockers (CCBs)/ACEi or ARB usage was associated with the lowest risk for composite outcome (OR, 0.86; 95% CI, 0.81-0.91 vs. TH/CCBs). The combinations of the ≥3 classes, including TH/CCB/ACEi or ARB, displayed the lowest odds for the composite outcome. In orthopaedic surgery and gastrointestinal resection, ACEis or ARBs were associated with better survival and physical function.
Conclusion: Perioperative use of ACEis or ARBs is associated with favourable outcomes in non-cardiac surgeries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


