{"title":"Ventilation distribution in mechanically ventilated children in response to positioning: An exploratory study.","authors":"A Lupton-Smith, A Argent, B Morrow","doi":"10.7196/SAJCC.2025.v41i1.2885","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Traditionally, it was understood that children universally show greater ventilation of the non-dependent lung. Recent studies have questioned the understanding of ventilation distribution patterns in the paediatric population. There are no studies examining the effect of body position in mechanically ventilated infants/children.</p><p><strong>Objectives: </strong>To determine the effect of body position on regional ventilation distribution in mechanically ventilated children.</p><p><strong>Methods: </strong>Thoracic electrical impedance tomography (EIT) measurements were taken in left- and right-side lying, supine and prone positions in mechanically ventilated infants/children. Functional EIT images were produced, and regional relative tidal impedance (ΔZ) in the left, right, ventral and dorsal lung regions was calculated. The proportion of ventilation occurring in large lung regions and regional filling were also calculated.</p><p><strong>Results: </strong>Seventeen children (n=8; 47% male) aged 6 months - 6 years are presented. Many of the children (n=8; 47%) consistently showed greater ventilation in the right lung in both side-lying positions, and in the dorsal lung region (n=6; 35%) in both the supine and prone positions. Regional filling was similar between lung regions in the different body positions.</p><p><strong>Conclusion: </strong>Ventilation distribution in mechanically ventilated infants/children with mild lung disease is variable and similar to that of healthy spontaneously breathing infants/children.</p><p><strong>Contribution of the study: </strong>Ventilation distribution in mechanically ventilated children with mild disease is not dissimilar to that in healthy infants and children. Positioning to optimise ventilation should be tailored to each child's responses. This study provides exploratory data describing ventilation distribution in mechanically ventilated infants and children. These data can be used to inform further research study design.</p>","PeriodicalId":75194,"journal":{"name":"The Southern African journal of critical care : the official journal of the Critical Care Society","volume":"41 1","pages":"e2885"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12378363/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Southern African journal of critical care : the official journal of the Critical Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7196/SAJCC.2025.v41i1.2885","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Traditionally, it was understood that children universally show greater ventilation of the non-dependent lung. Recent studies have questioned the understanding of ventilation distribution patterns in the paediatric population. There are no studies examining the effect of body position in mechanically ventilated infants/children.
Objectives: To determine the effect of body position on regional ventilation distribution in mechanically ventilated children.
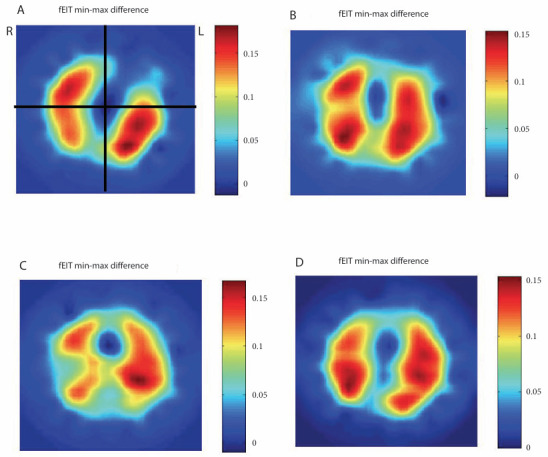
Methods: Thoracic electrical impedance tomography (EIT) measurements were taken in left- and right-side lying, supine and prone positions in mechanically ventilated infants/children. Functional EIT images were produced, and regional relative tidal impedance (ΔZ) in the left, right, ventral and dorsal lung regions was calculated. The proportion of ventilation occurring in large lung regions and regional filling were also calculated.
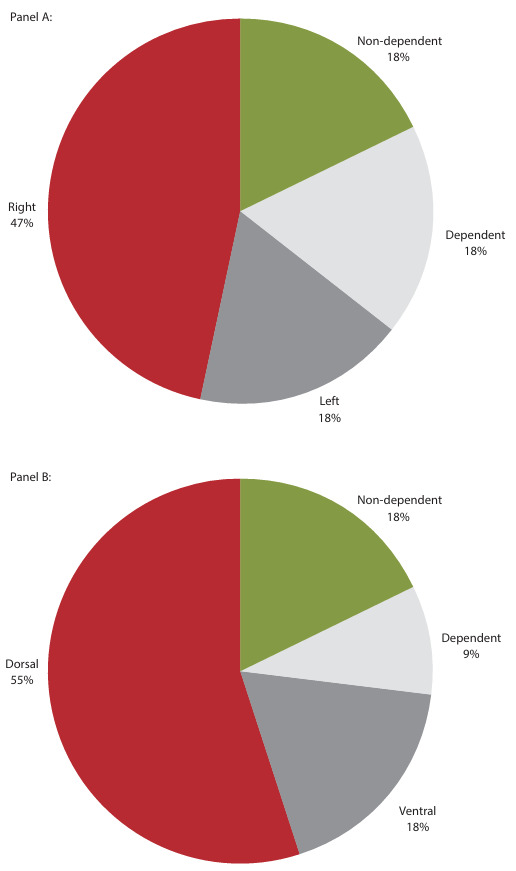
Results: Seventeen children (n=8; 47% male) aged 6 months - 6 years are presented. Many of the children (n=8; 47%) consistently showed greater ventilation in the right lung in both side-lying positions, and in the dorsal lung region (n=6; 35%) in both the supine and prone positions. Regional filling was similar between lung regions in the different body positions.
Conclusion: Ventilation distribution in mechanically ventilated infants/children with mild lung disease is variable and similar to that of healthy spontaneously breathing infants/children.
Contribution of the study: Ventilation distribution in mechanically ventilated children with mild disease is not dissimilar to that in healthy infants and children. Positioning to optimise ventilation should be tailored to each child's responses. This study provides exploratory data describing ventilation distribution in mechanically ventilated infants and children. These data can be used to inform further research study design.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


