{"title":"Gestational Diabetes Mellitus: The Dual Risk of Small and Large for Gestational Age: A Narrative Review.","authors":"Andreea Fotă, Aida Petca","doi":"10.3390/medsci13030144","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background/Objectives</b>: Gestational diabetes mellitus (GDM) complicates approximately 14% of pregnancies worldwide, its prevalence rising with increasing maternal age and obesity. While maternal hyperglycemia is traditionally associated with fetal overgrowth and large-for-gestational-age (LGA) neonates, emerging evidence indicates that GDM may also contribute to small-for-gestational-age (SGA) outcomes. <b>Methods</b>: A comprehensive literature search was conducted using multiple databases, including PubMed, Web of Science, and ScienceDirect, to identify studies related to gestational diabetes mellitus, fetal growth outcomes such as small for gestational age and large for gestational age, and associated pathophysiological mechanisms. <b>Results</b>: This narrative review explores the mechanisms by which GDM influences fetal growth, emphasizing the dual risk of excessive and restricted intrauterine growth. Fetal macrosomia typically results from chronic maternal hyperglycemia, leading to increased transplacental glucose delivery and fetal hyperinsulinemia. In contrast, SGA outcomes are a consequence of vascular and endothelial dysfunction, placental insufficiency, or excessively restrictive glycemic control that limit the availability of nutrients. Both extremes of fetal growth carry a myriad of significant perinatal and long-term metabolic risks. <b>Conclusions</b>: Understanding the diverse pathways through which GDM affects fetal growth is essential for developing individualized clinical strategies.</p>","PeriodicalId":74152,"journal":{"name":"Medical sciences (Basel, Switzerland)","volume":"13 3","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372126/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical sciences (Basel, Switzerland)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/medsci13030144","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
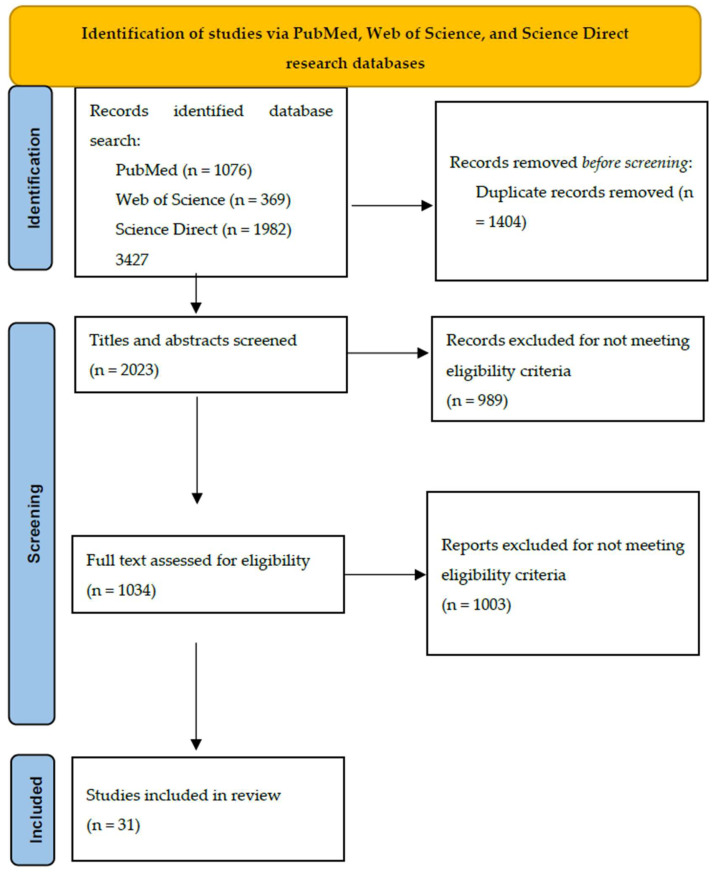
Background/Objectives: Gestational diabetes mellitus (GDM) complicates approximately 14% of pregnancies worldwide, its prevalence rising with increasing maternal age and obesity. While maternal hyperglycemia is traditionally associated with fetal overgrowth and large-for-gestational-age (LGA) neonates, emerging evidence indicates that GDM may also contribute to small-for-gestational-age (SGA) outcomes. Methods: A comprehensive literature search was conducted using multiple databases, including PubMed, Web of Science, and ScienceDirect, to identify studies related to gestational diabetes mellitus, fetal growth outcomes such as small for gestational age and large for gestational age, and associated pathophysiological mechanisms. Results: This narrative review explores the mechanisms by which GDM influences fetal growth, emphasizing the dual risk of excessive and restricted intrauterine growth. Fetal macrosomia typically results from chronic maternal hyperglycemia, leading to increased transplacental glucose delivery and fetal hyperinsulinemia. In contrast, SGA outcomes are a consequence of vascular and endothelial dysfunction, placental insufficiency, or excessively restrictive glycemic control that limit the availability of nutrients. Both extremes of fetal growth carry a myriad of significant perinatal and long-term metabolic risks. Conclusions: Understanding the diverse pathways through which GDM affects fetal growth is essential for developing individualized clinical strategies.
背景/目的:妊娠期糖尿病(GDM)在全世界约占妊娠并发症的14%,其患病率随着产妇年龄和肥胖的增加而上升。虽然母体高血糖通常与胎儿过度生长和大胎龄(LGA)新生儿有关,但新出现的证据表明,GDM也可能导致小胎龄(SGA)结局。方法:通过PubMed、Web of Science、ScienceDirect等多个数据库进行综合文献检索,确定与妊娠期糖尿病、胎龄小、胎龄大等胎儿生长结局及相关病理生理机制相关的研究。结果:这篇叙述性综述探讨了GDM影响胎儿生长的机制,强调了过度和限制性宫内生长的双重风险。胎儿巨大症通常由母体慢性高血糖引起,导致经胎盘葡萄糖输送增加和胎儿高胰岛素血症。相反,SGA的结果是血管和内皮功能障碍、胎盘功能不全或过度限制血糖控制的结果,这些限制了营养物质的可用性。这两种极端的胎儿生长都带来了无数重大的围产期和长期代谢风险。结论:了解GDM影响胎儿生长的多种途径对于制定个性化的临床策略至关重要。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


