Raphaëlle Giguère, Victor Niaussat, Monia Noël-Hunter, William Witteman, Tanya S Paul, Alexandre Marois, Philippe Després, Simon Duchesne, Patrick M Archambault
{"title":"Predicting Episodes of Hypovigilance in Intensive Care Units Using Routine Physiological Parameters and Artificial Intelligence: Derivation Study.","authors":"Raphaëlle Giguère, Victor Niaussat, Monia Noël-Hunter, William Witteman, Tanya S Paul, Alexandre Marois, Philippe Després, Simon Duchesne, Patrick M Archambault","doi":"10.2196/60885","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Delirium is prevalent in intensive care units (ICUs), often leading to adverse outcomes. Hypoactive delirium is particularly difficult to detect. Despite the development of new tools, the timely identification of hypoactive delirium remains clinically challenging due to its dynamic nature, lack of human resources, lack of reliable monitoring tools, and subtle clinical signs including hypovigilance. Machine learning models could support the identification of hypoactive delirium episodes by better detecting episodes of hypovigilance.</p><p><strong>Objective: </strong>Develop an artificial intelligence prediction model capable of detecting hypovigilance events using routinely collected physiological data in the ICU.</p><p><strong>Methods: </strong>This derivation study was conducted using data from a prospective observational cohort of eligible patients admitted to the ICU in Lévis, Québec, Canada. We included patients admitted to the ICU between October 2021 and June 2022 who were aged ≥18 years and had an anticipated ICU stay of ≥48 hours. ICU nurses identified hypovigilant states every hour using the Richmond Agitation and Sedation Scale (RASS) or the Ramsay Sedation Scale (RSS). Routine vital signs (heart rate, respiratory rate, blood pressure, and oxygen saturation), as well as other physiological and clinical variables (premature ventricular contractions, intubation, use of sedative medication, and temperature), were automatically collected and stored using a CARESCAPE Gateway (General Electric) or manually collected (for sociodemographic characteristics and medication) through chart review. Time series were generated around hypovigilance episodes for analysis. Random Forest, XGBoost, and Light Gradient Boosting Machine classifiers were then used to detect hypovigilant episodes based on time series analysis. Hyperparameter optimization was performed using a random search in a 10-fold group-based cross-validation setup. To interpret the predictions of the best-performing models, we conducted a Shapley Additive Explanations (SHAP) analysis. We report the results of this study using the TRIPOD+AI (Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis for machine learning models) guidelines, and potential biases were assessed using PROBAST (Prediction model Risk Of Bias ASsessment Tool).</p><p><strong>Results: </strong>Out of 136 potentially eligible participants, data from 30 patients (mean age 69 y, 63% male) were collected for analysis. Among all participants, 30% were admitted to the ICU for surgical reasons. Following data preprocessing, the study included 1493 hypovigilance episodes and 764 nonhypovigilant episodes. Among the 3 models evaluated, Light Gradient Boosting Machine demonstrated the best performance. It achieved an average accuracy of 68% to detect hypovigilant episodes, with a precision of 76%, a recall of 74%, an area under the curve (AUC) of 60%, and an F1-score of 69%. SHAP analysis revealed that intubation status, respiratory rate, and noninvasive systolic blood pressure were the primary drivers of the model's predictions.</p><p><strong>Conclusions: </strong>All classifiers produced precision and recall values that show potential for further development, with slightly different yet comparable performances in classifying hypovigilant episodes. Machine learning algorithms designed to detect hypovigilance have the potential to support early detection of hypoactive delirium in patients in the ICU.</p>","PeriodicalId":73551,"journal":{"name":"JMIR AI","volume":"4 ","pages":"e60885"},"PeriodicalIF":2.0000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12384691/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR AI","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/60885","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Delirium is prevalent in intensive care units (ICUs), often leading to adverse outcomes. Hypoactive delirium is particularly difficult to detect. Despite the development of new tools, the timely identification of hypoactive delirium remains clinically challenging due to its dynamic nature, lack of human resources, lack of reliable monitoring tools, and subtle clinical signs including hypovigilance. Machine learning models could support the identification of hypoactive delirium episodes by better detecting episodes of hypovigilance.
Objective: Develop an artificial intelligence prediction model capable of detecting hypovigilance events using routinely collected physiological data in the ICU.
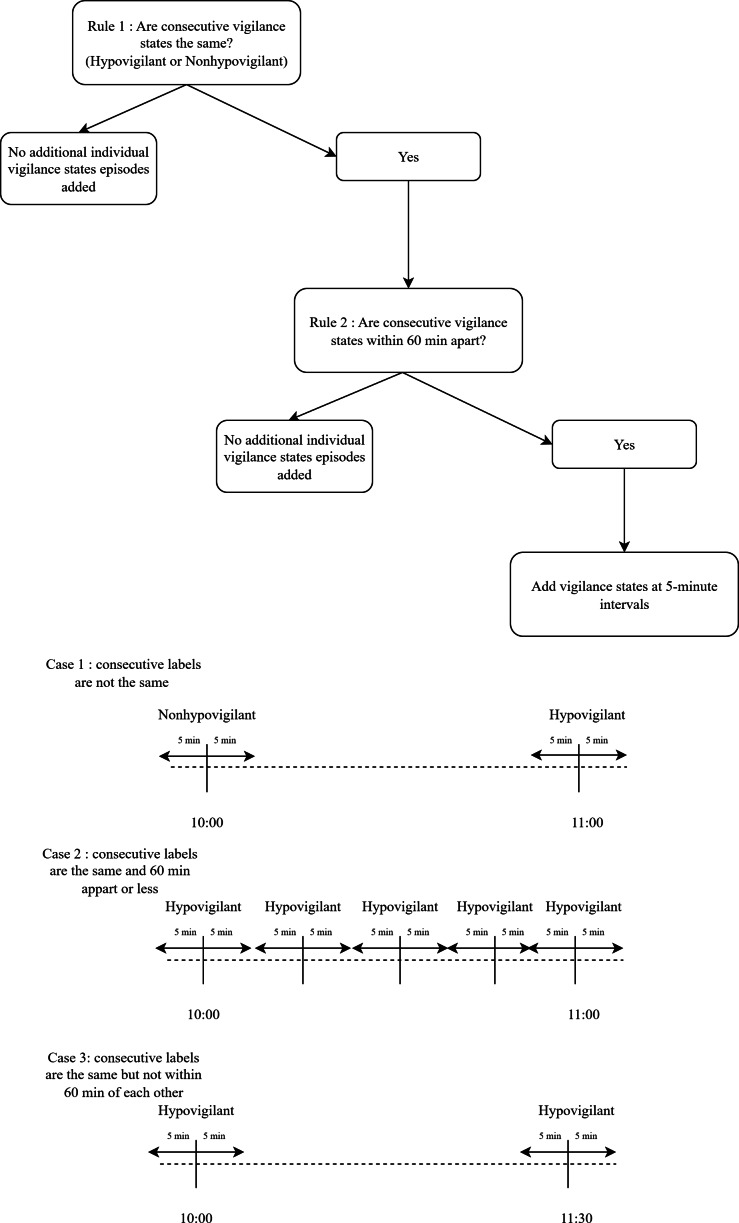
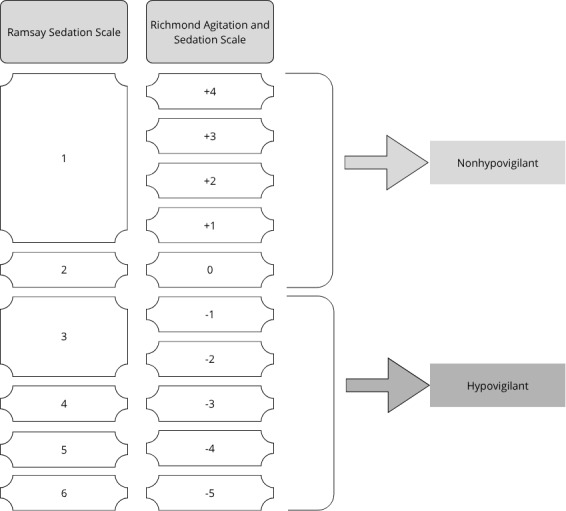
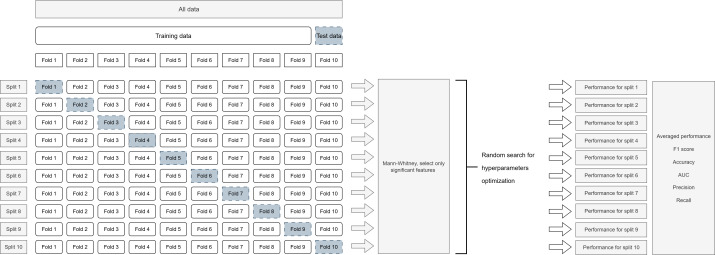
Methods: This derivation study was conducted using data from a prospective observational cohort of eligible patients admitted to the ICU in Lévis, Québec, Canada. We included patients admitted to the ICU between October 2021 and June 2022 who were aged ≥18 years and had an anticipated ICU stay of ≥48 hours. ICU nurses identified hypovigilant states every hour using the Richmond Agitation and Sedation Scale (RASS) or the Ramsay Sedation Scale (RSS). Routine vital signs (heart rate, respiratory rate, blood pressure, and oxygen saturation), as well as other physiological and clinical variables (premature ventricular contractions, intubation, use of sedative medication, and temperature), were automatically collected and stored using a CARESCAPE Gateway (General Electric) or manually collected (for sociodemographic characteristics and medication) through chart review. Time series were generated around hypovigilance episodes for analysis. Random Forest, XGBoost, and Light Gradient Boosting Machine classifiers were then used to detect hypovigilant episodes based on time series analysis. Hyperparameter optimization was performed using a random search in a 10-fold group-based cross-validation setup. To interpret the predictions of the best-performing models, we conducted a Shapley Additive Explanations (SHAP) analysis. We report the results of this study using the TRIPOD+AI (Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis for machine learning models) guidelines, and potential biases were assessed using PROBAST (Prediction model Risk Of Bias ASsessment Tool).
Results: Out of 136 potentially eligible participants, data from 30 patients (mean age 69 y, 63% male) were collected for analysis. Among all participants, 30% were admitted to the ICU for surgical reasons. Following data preprocessing, the study included 1493 hypovigilance episodes and 764 nonhypovigilant episodes. Among the 3 models evaluated, Light Gradient Boosting Machine demonstrated the best performance. It achieved an average accuracy of 68% to detect hypovigilant episodes, with a precision of 76%, a recall of 74%, an area under the curve (AUC) of 60%, and an F1-score of 69%. SHAP analysis revealed that intubation status, respiratory rate, and noninvasive systolic blood pressure were the primary drivers of the model's predictions.
Conclusions: All classifiers produced precision and recall values that show potential for further development, with slightly different yet comparable performances in classifying hypovigilant episodes. Machine learning algorithms designed to detect hypovigilance have the potential to support early detection of hypoactive delirium in patients in the ICU.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


