Bridging Global Disparities in Breast Cancer Care: External Validation Study of the MD Anderson "Nomogram To Predict Positive Sentinel Lymph Nodes After Neoadjuvant Chemotherapy" and Its Financial Implications of Axillary De-escalation in a Resource Limited Setting.
{"title":"Bridging Global Disparities in Breast Cancer Care: External Validation Study of the MD Anderson \"Nomogram To Predict Positive Sentinel Lymph Nodes After Neoadjuvant Chemotherapy\" and Its Financial Implications of Axillary De-escalation in a Resource Limited Setting.","authors":"Vishal Farid Raza, Ayesha Ehsan, Amina Iqbal Khan","doi":"10.1177/00469580251366150","DOIUrl":null,"url":null,"abstract":"<p><p>Axillary surgery in breast cancer has evolved from radical dissections to selective de-escalations. Identifying patients who may safely omit sentinel lymph node biopsy (SLNB) can further reduce the surgical burden, post operative complications and financial toxicity associated with breast cancer surgical care. The MD Anderson \"Nomogram To Predict Positive Sentinel Lymph Nodes After Neoadjuvant Chemotherapy\" is widely available and free of charge to assess SLNB positivity post neoadjuvant chemotherapy (NACT). This study externally validates its accuracy in a sample of Pakistani women and assesses its implications for cost effective breast cancer care in a resource limited setting. Retrospective chart review of 150 women who underwent axillary sentinel lymph node biopsy post NACT at Shaukat Khanum Memorial Cancer Hospital from January 2023 to August 2024. Predicted node probability and observed positivity on histopathology were recorded. Calibration (Hosmer-Lemeshow test) and discrimination (C-index) were calculated. 98% were ductal carcinomas; tumor sub-types showed luminal A (42.7%), luminal B (4.7%), her2neu (H2N) enriched (14%) and triple negative (TNBC; 38.7%). 18% (n = 27) nodes were positive on final pathology closely aligning with the nomogram's predicted probability of 17.1 ± 10.3%. Calibration showed good model fit (<i>P</i> = .89) while C-index (0.64) indicated moderate discrimination. 12.6% of women would avoid costs of SLNB if omitted in the 0% to 5% bracket and 31.3% of women in the 0% to 10% bracket. TNBC demonstrated lowest positivity of 6.89% (<i>P</i> = .01). The MD Anderson Clinical Calculator for predicting positive sentinel lymph nodes post NACT may have a role in tailoring decisions for axillary de-escalation especially in patients with a low probability score between 0% and 10% with decrease in costs of breast cancer care in LMICs. Future studies incorporating safety of axillary surgery omission using the calculator and its economic impact are warranted.</p>","PeriodicalId":54976,"journal":{"name":"Inquiry-The Journal of Health Care Organization Provision and Financing","volume":"62 ","pages":"469580251366150"},"PeriodicalIF":2.3000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374028/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Inquiry-The Journal of Health Care Organization Provision and Financing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/00469580251366150","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/21 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
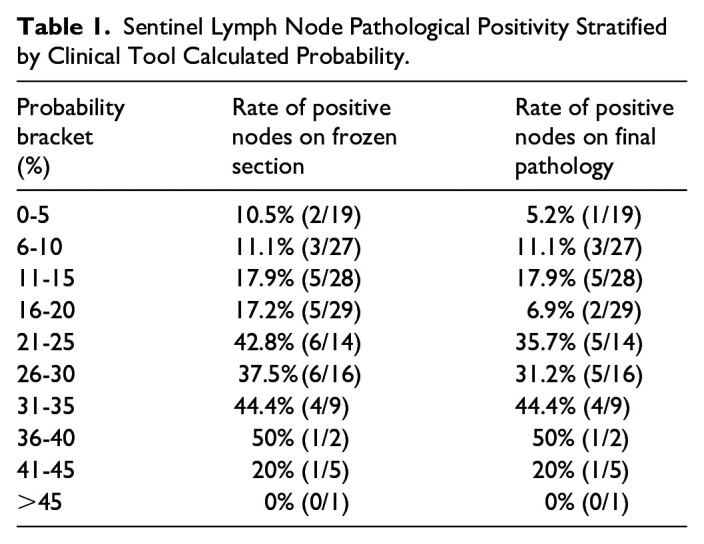
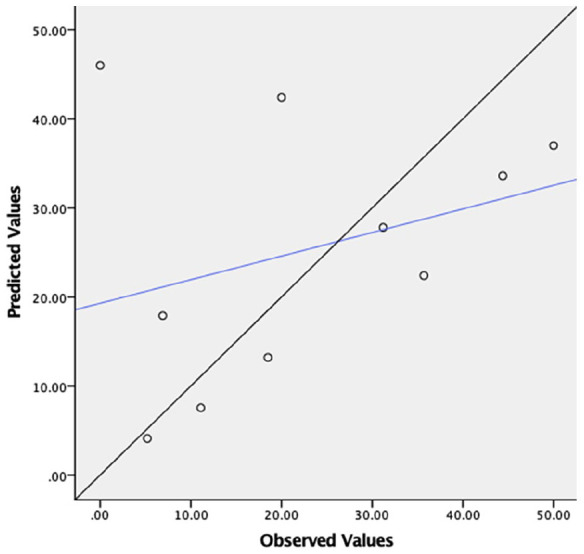
Axillary surgery in breast cancer has evolved from radical dissections to selective de-escalations. Identifying patients who may safely omit sentinel lymph node biopsy (SLNB) can further reduce the surgical burden, post operative complications and financial toxicity associated with breast cancer surgical care. The MD Anderson "Nomogram To Predict Positive Sentinel Lymph Nodes After Neoadjuvant Chemotherapy" is widely available and free of charge to assess SLNB positivity post neoadjuvant chemotherapy (NACT). This study externally validates its accuracy in a sample of Pakistani women and assesses its implications for cost effective breast cancer care in a resource limited setting. Retrospective chart review of 150 women who underwent axillary sentinel lymph node biopsy post NACT at Shaukat Khanum Memorial Cancer Hospital from January 2023 to August 2024. Predicted node probability and observed positivity on histopathology were recorded. Calibration (Hosmer-Lemeshow test) and discrimination (C-index) were calculated. 98% were ductal carcinomas; tumor sub-types showed luminal A (42.7%), luminal B (4.7%), her2neu (H2N) enriched (14%) and triple negative (TNBC; 38.7%). 18% (n = 27) nodes were positive on final pathology closely aligning with the nomogram's predicted probability of 17.1 ± 10.3%. Calibration showed good model fit (P = .89) while C-index (0.64) indicated moderate discrimination. 12.6% of women would avoid costs of SLNB if omitted in the 0% to 5% bracket and 31.3% of women in the 0% to 10% bracket. TNBC demonstrated lowest positivity of 6.89% (P = .01). The MD Anderson Clinical Calculator for predicting positive sentinel lymph nodes post NACT may have a role in tailoring decisions for axillary de-escalation especially in patients with a low probability score between 0% and 10% with decrease in costs of breast cancer care in LMICs. Future studies incorporating safety of axillary surgery omission using the calculator and its economic impact are warranted.
期刊介绍:
INQUIRY is a peer-reviewed open access journal whose msision is to to improve health by sharing research spanning health care, including public health, health services, and health policy.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


