Lei Hu, Chuan Wang, Zhongqin Zhou, Shiganmo Azhe, Shengkun Peng, Nanjun Zhang, Kaiyu Zhou, Yingkun Guo, Li Yu, Lingyi Wen
{"title":"Comprehensive assessment of patients with Kawasaki disease without coronary artery aneurysm.","authors":"Lei Hu, Chuan Wang, Zhongqin Zhou, Shiganmo Azhe, Shengkun Peng, Nanjun Zhang, Kaiyu Zhou, Yingkun Guo, Li Yu, Lingyi Wen","doi":"10.21037/qims-2024-2772","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In the current guidelines, the management algorithm for patients with Kawasaki disease (KD) without coronary artery (CA) aneurysms primarily depends on the clinical experience of pediatricians. It is necessary to conduct a comprehensive evaluation of these patients to provide a higher level of evidence for their management. Therefore, our study aimed to assess patients with KD using multidimensional data and investigate their prognosis.</p><p><strong>Methods: </strong>A total of 455 patients with KD were retrospectively recruited and divided into a non-CA involvement group (n=313) and a CA dilation-only group (n=142), with 16.1% (50/311) and 15.5% (22/142), respectively, undergoing cardiac magnetic resonance (CMR) examinations during recovery. Data regarding inflammatory markers, electrocardiography, and echocardiography were compared between the two groups both in the acute phase and during the recovery period. Kaplan-Meier analysis was performed to estimate the cumulative probability of the endpoints including coronary events, cardiac death, heart failure, and new-onset malignant arrhythmias.</p><p><strong>Results: </strong>Baseline inflammatory markers, including white blood cell count (WBC) and C-reactive protein (CRP), were not significantly different between patients with KD and non-CA involvement and those with dilation only (median WBC: 14.1×10<sup>9</sup>/L <i>vs.</i> 13.9×10<sup>9</sup>/L, P=0.57; median CRP: 87.4 <i>vs.</i> 85.6 mg/L, P=0.73). In terms of echocardiography assessment at baseline, there were no significant differences between the non-CA involvement group and the dilation-only group in terms of left ventricular ejection fraction (67.8%±13.6% <i>vs.</i> 68.1%±10.3%; P=0.13) or fractional shortening (37.6%±5.3% <i>vs.</i> 35.4%±6.6%; P=0.25). For CMR assessment at recovery, the myocardial systolic function of patients with KD but non-CA involvement was not significantly different from that of patients with CA dilation only in terms of global radial strain (38.3%±18.7% <i>vs.</i> 39.9%±20.5%; P=0.20), global circumferential strain (-18.7%±6.8% <i>vs.</i> -18.3%±7.2%; P=0.38), and global longitudinal strain (-13.2%±3.7% <i>vs.</i> -13.4%±4.1%; P=0.17). The global native T1 value of patients with non-CA involvement was 1,296.5±74.1 msec, while that of patients with CA dilation only was 1,313.3±80.5 msec (P=0.21); there was also no significant difference in global T2 values between the two groups of patients (38.2±4.1 <i>vs.</i> 38.1±3.5 msec; P=0.53). Finally, at a median follow-up of 4.2 years, there was a favorable prognosis in both two groups of patients, with no patients reaching the endpoints.</p><p><strong>Conclusions: </strong>Comprehensive assessment revealed no significant differences between patients with KD and CA dilation only and those with non-CA involvement, and thus these patients should be treated according to the same medium-long-term management algorithm.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 9","pages":"8348-8358"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397668/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-2024-2772","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In the current guidelines, the management algorithm for patients with Kawasaki disease (KD) without coronary artery (CA) aneurysms primarily depends on the clinical experience of pediatricians. It is necessary to conduct a comprehensive evaluation of these patients to provide a higher level of evidence for their management. Therefore, our study aimed to assess patients with KD using multidimensional data and investigate their prognosis.
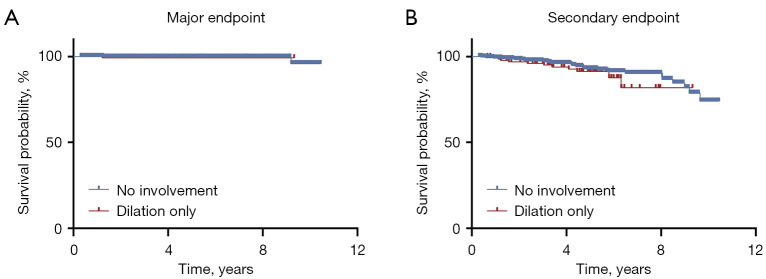
Methods: A total of 455 patients with KD were retrospectively recruited and divided into a non-CA involvement group (n=313) and a CA dilation-only group (n=142), with 16.1% (50/311) and 15.5% (22/142), respectively, undergoing cardiac magnetic resonance (CMR) examinations during recovery. Data regarding inflammatory markers, electrocardiography, and echocardiography were compared between the two groups both in the acute phase and during the recovery period. Kaplan-Meier analysis was performed to estimate the cumulative probability of the endpoints including coronary events, cardiac death, heart failure, and new-onset malignant arrhythmias.
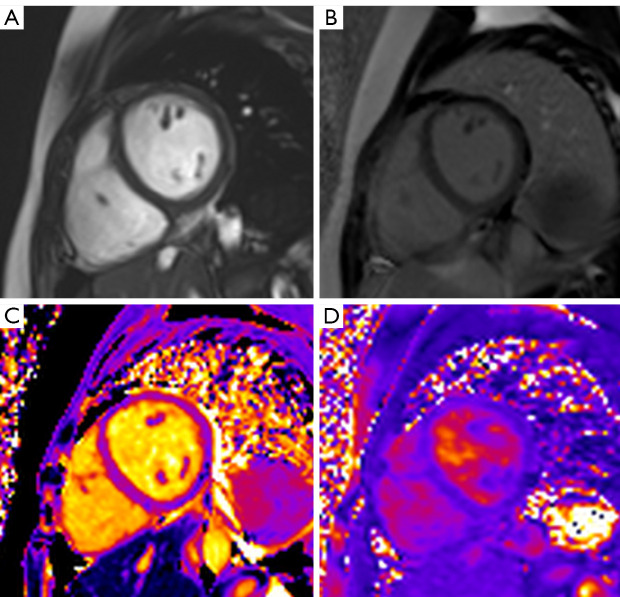
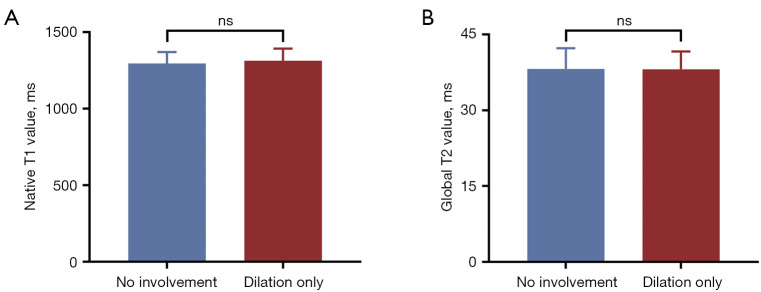
Results: Baseline inflammatory markers, including white blood cell count (WBC) and C-reactive protein (CRP), were not significantly different between patients with KD and non-CA involvement and those with dilation only (median WBC: 14.1×109/L vs. 13.9×109/L, P=0.57; median CRP: 87.4 vs. 85.6 mg/L, P=0.73). In terms of echocardiography assessment at baseline, there were no significant differences between the non-CA involvement group and the dilation-only group in terms of left ventricular ejection fraction (67.8%±13.6% vs. 68.1%±10.3%; P=0.13) or fractional shortening (37.6%±5.3% vs. 35.4%±6.6%; P=0.25). For CMR assessment at recovery, the myocardial systolic function of patients with KD but non-CA involvement was not significantly different from that of patients with CA dilation only in terms of global radial strain (38.3%±18.7% vs. 39.9%±20.5%; P=0.20), global circumferential strain (-18.7%±6.8% vs. -18.3%±7.2%; P=0.38), and global longitudinal strain (-13.2%±3.7% vs. -13.4%±4.1%; P=0.17). The global native T1 value of patients with non-CA involvement was 1,296.5±74.1 msec, while that of patients with CA dilation only was 1,313.3±80.5 msec (P=0.21); there was also no significant difference in global T2 values between the two groups of patients (38.2±4.1 vs. 38.1±3.5 msec; P=0.53). Finally, at a median follow-up of 4.2 years, there was a favorable prognosis in both two groups of patients, with no patients reaching the endpoints.
Conclusions: Comprehensive assessment revealed no significant differences between patients with KD and CA dilation only and those with non-CA involvement, and thus these patients should be treated according to the same medium-long-term management algorithm.
背景:在目前的指南中,川崎病(KD)无冠状动脉(CA)动脉瘤患者的治疗算法主要取决于儿科医生的临床经验。有必要对这些患者进行综合评价,为其治疗提供更高水平的依据。因此,我们的研究旨在利用多维数据评估KD患者并探讨其预后。方法:回顾性招募455例KD患者,分为非CA受累组(n=313)和CA扩张组(n=142),分别有16.1%(50/311)和15.5%(22/142)患者在康复期间接受心脏磁共振(CMR)检查。比较两组急性期和恢复期的炎症标志物、心电图和超声心动图数据。采用Kaplan-Meier分析来估计终点的累积概率,包括冠状动脉事件、心源性死亡、心力衰竭和新发恶性心律失常。结果:基线炎症标志物,包括白细胞计数(WBC)和c反应蛋白(CRP),在KD和非ca累及患者与仅扩张患者之间无显著差异(WBC中位数:14.1×109/L vs 13.9×109/L, P=0.57; CRP中位数:87.4 vs 85.6 mg/L, P=0.73)。在基线超声心动图评估方面,在左心室射血分数(67.8%±13.6% vs 68.1%±10.3%;P=0.13)或分数缩短(37.6%±5.3% vs 35.4%±6.6%;P=0.25)方面,非ca受累组和仅扩张术组之间没有显著差异。对于恢复时的CMR评估,KD但不累及CA的患者的心肌收缩功能与仅CA扩张的患者在总径向应变(38.3%±18.7% vs. 39.9%±20.5%,P=0.20)、总周向应变(-18.7%±6.8% vs. -18.3%±7.2%,P=0.38)和总纵向应变(-13.2%±3.7% vs. -13.4%±4.1%,P=0.17)方面无显著差异。无CA累及患者的整体原生T1值为1296.5±74.1 msec,仅CA扩张患者的T1值为1313.3±80.5 msec (P=0.21);两组患者的总T2值也无显著差异(38.2±4.1 vs 38.1±3.5 msec; P=0.53)。最后,中位随访4.2年,两组患者预后良好,均无患者达到终点。结论:综合评估显示仅KD和CA扩张的患者与不累及CA的患者之间无显著差异,因此这些患者应按照相同的中长期管理算法进行治疗。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


