Value of high-density lipoprotein cholesterol, myocardial perfusion index, and global longitudinal strain derived from cardiac magnetic resonance imaging in predicting coronary slow flow in patients with nonobstructive coronary artery disease.
IF 2.3 2区 医学Q2 RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
{"title":"Value of high-density lipoprotein cholesterol, myocardial perfusion index, and global longitudinal strain derived from cardiac magnetic resonance imaging in predicting coronary slow flow in patients with nonobstructive coronary artery disease.","authors":"Yunbo Zhang, Lin Sun, Xin-Xiang Zhao","doi":"10.21037/qims-24-1668","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Coronary slow flow (CSF) is associated with dyslipidemias, smoking, and increased body mass index (BMI), yet its diagnosis through noninvasive methods remains challenging. Cardiac magnetic resonance (CMR) is a multimodal imaging technique that enables the simultaneous assessment of impaired myocardial perfusion and deteriorated ventricular function in patients with cardiac disease. This study aimed to demonstrate altered perfusion and deformation parameters on CMR and to evaluate the value of CMR parameters for predicting CSF.</p><p><strong>Methods: </strong>Participants without obstructive epicardial arterial disease who underwent CMR imaging and coronary angiography (CAG) for typical angina symptoms were enrolled in this retrospective study. CSF was defined by the presence of at least one CAG showing corrected thrombolysis in myocardial infarction frame count (CTFC) >27 frames. The myocardial perfusion index (PI) was analyzed via semiquantitative resting first-pass perfusion. Left ventricular (LV) performance was assessed via CMR feature tracking (CMR-FT) cine imaging, including global longitudinal strain (GLS), global circumferential strain (GCS), and global radial strain (GRS). Baseline clinical factors were collected, including sex, age, and traditional cardiovascular risk factors, along with levels of low-density lipoprotein cholesterol, high-density lipoprotein cholesterol (HDL-C), triglyceride (TG), and serum creatinine. Multivariate logistic regression analysis was performed to identify independent predictors of CSF, and a combined prediction model for CSF was developed. The predictive accuracy of the parameters was evaluated via receiver operating characteristic (ROC) curves.</p><p><strong>Results: </strong>A total of 146 participants who underwent CAG and CMR were included and divided into CSF (n=73; 78.1% male; age 49.44±9.59 years) and control (n=73; 57.5% male; age 47.32±13.57 years) groups based on CTFC. Patients with CSF were more likely to have a higher BMI, hyperuricemia, peripheral arterial disease, and a smoking habit, as well as lower HDL-C levels and elevated TGs as compared to controls. Compared with controls, patients with CSF had impaired GLS (-12.09%±2.69% <i>vs</i>. -14.38%±2.36%) and GCS (-18.70%±3.24% <i>vs</i>. -19.80%±2.21%) (all P values <0.05). Global LV PI was significantly decreased in patients with CSF as compared with controls (11.34%±4.24% <i>vs</i>. 15.25%±8.50%; P<0.001). After adjustments were made for clinical factors and imaging indices, multivariate analysis indicated that the independent predictors of CSF were HDL-C [odds ratio (OR) 0.119; 95% confidence interval (CI): 0.016-0.897; P=0.039], GLS (OR 1.339; 95% CI: 1.112-1.613; P=0.002), and global LV PI (OR 0.456; 95% CI: 0.209-0.994; P=0.048). Moreover, in predicting CSF, the combination of PI, GLS, and HDL-C yielded the best area under the curve (with an 84.9% sensitivity and a 60.3% specificity) as compared to PI (0.783 <i>vs</i>. 0.616; P<0.001), GLS (0.783 <i>vs</i>. 0.742; P=0.130), and HDL-C (0.783 <i>vs</i>. 0.654; P=0.003), respectively.</p><p><strong>Conclusions: </strong>Reduced HDL-C, decreased PI, and GLS derived from CMR may serve as predictors of CSF. Further multicenter, randomized controlled trials with larger sample sizes are needed to validate these findings.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 9","pages":"8491-8504"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397633/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-24-1668","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/11 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Coronary slow flow (CSF) is associated with dyslipidemias, smoking, and increased body mass index (BMI), yet its diagnosis through noninvasive methods remains challenging. Cardiac magnetic resonance (CMR) is a multimodal imaging technique that enables the simultaneous assessment of impaired myocardial perfusion and deteriorated ventricular function in patients with cardiac disease. This study aimed to demonstrate altered perfusion and deformation parameters on CMR and to evaluate the value of CMR parameters for predicting CSF.
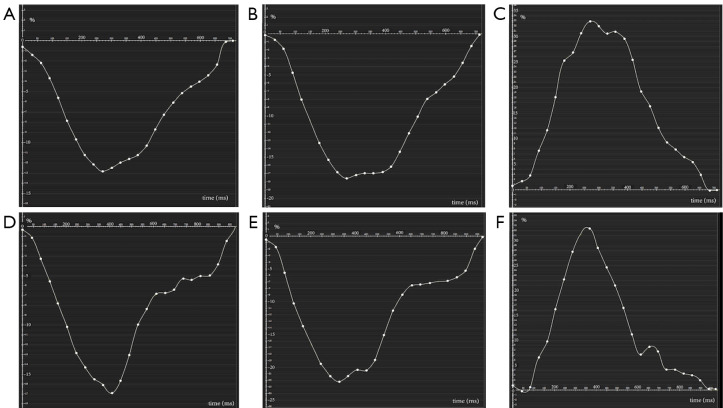
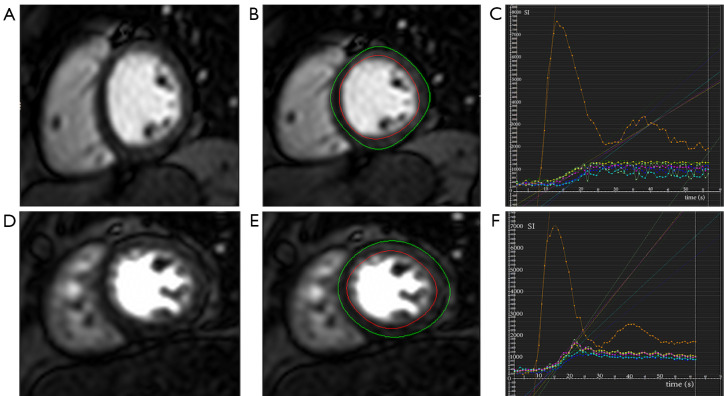
Methods: Participants without obstructive epicardial arterial disease who underwent CMR imaging and coronary angiography (CAG) for typical angina symptoms were enrolled in this retrospective study. CSF was defined by the presence of at least one CAG showing corrected thrombolysis in myocardial infarction frame count (CTFC) >27 frames. The myocardial perfusion index (PI) was analyzed via semiquantitative resting first-pass perfusion. Left ventricular (LV) performance was assessed via CMR feature tracking (CMR-FT) cine imaging, including global longitudinal strain (GLS), global circumferential strain (GCS), and global radial strain (GRS). Baseline clinical factors were collected, including sex, age, and traditional cardiovascular risk factors, along with levels of low-density lipoprotein cholesterol, high-density lipoprotein cholesterol (HDL-C), triglyceride (TG), and serum creatinine. Multivariate logistic regression analysis was performed to identify independent predictors of CSF, and a combined prediction model for CSF was developed. The predictive accuracy of the parameters was evaluated via receiver operating characteristic (ROC) curves.
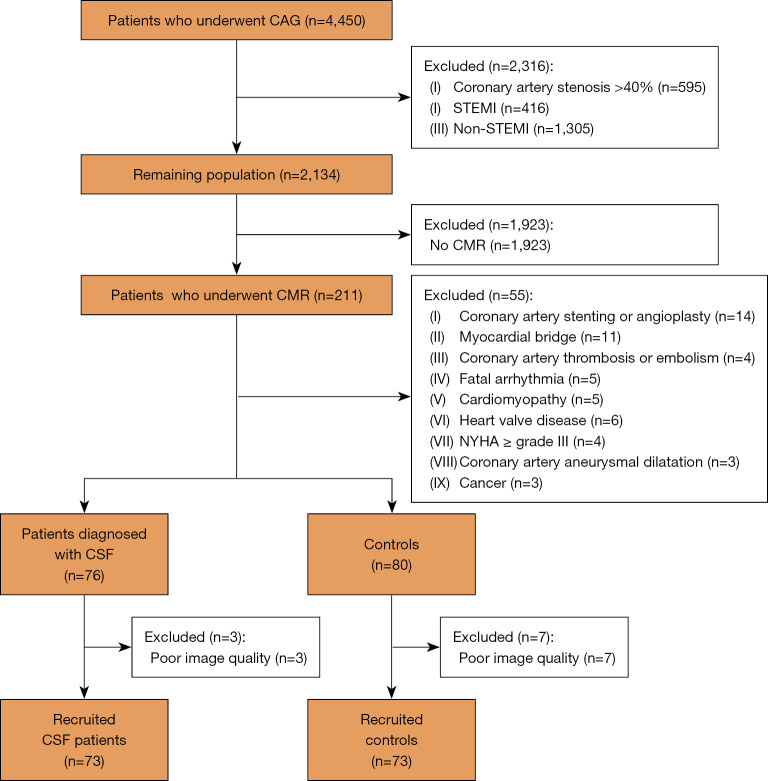
Results: A total of 146 participants who underwent CAG and CMR were included and divided into CSF (n=73; 78.1% male; age 49.44±9.59 years) and control (n=73; 57.5% male; age 47.32±13.57 years) groups based on CTFC. Patients with CSF were more likely to have a higher BMI, hyperuricemia, peripheral arterial disease, and a smoking habit, as well as lower HDL-C levels and elevated TGs as compared to controls. Compared with controls, patients with CSF had impaired GLS (-12.09%±2.69% vs. -14.38%±2.36%) and GCS (-18.70%±3.24% vs. -19.80%±2.21%) (all P values <0.05). Global LV PI was significantly decreased in patients with CSF as compared with controls (11.34%±4.24% vs. 15.25%±8.50%; P<0.001). After adjustments were made for clinical factors and imaging indices, multivariate analysis indicated that the independent predictors of CSF were HDL-C [odds ratio (OR) 0.119; 95% confidence interval (CI): 0.016-0.897; P=0.039], GLS (OR 1.339; 95% CI: 1.112-1.613; P=0.002), and global LV PI (OR 0.456; 95% CI: 0.209-0.994; P=0.048). Moreover, in predicting CSF, the combination of PI, GLS, and HDL-C yielded the best area under the curve (with an 84.9% sensitivity and a 60.3% specificity) as compared to PI (0.783 vs. 0.616; P<0.001), GLS (0.783 vs. 0.742; P=0.130), and HDL-C (0.783 vs. 0.654; P=0.003), respectively.
Conclusions: Reduced HDL-C, decreased PI, and GLS derived from CMR may serve as predictors of CSF. Further multicenter, randomized controlled trials with larger sample sizes are needed to validate these findings.
背景:冠状动脉慢血流(CSF)与血脂异常、吸烟和体重指数(BMI)增加有关,但通过无创方法诊断仍具有挑战性。心脏磁共振(CMR)是一种多模态成像技术,可以同时评估心脏病患者的心肌灌注受损和心室功能恶化。本研究旨在证明CMR灌注和变形参数的改变,并评估CMR参数预测CSF的价值。方法:没有梗阻性心外膜动脉疾病的参与者接受了典型心绞痛症状的CMR成像和冠状动脉造影(CAG),纳入了这项回顾性研究。CSF的定义是在心肌梗死帧数(CTFC)中至少有一个CAG显示纠正的溶栓。采用半定量静息首过灌注法分析心肌灌注指数(PI)。通过CMR特征跟踪(CMR- ft)电影成像评估左心室(LV)的表现,包括整体纵向应变(GLS)、整体圆周应变(GCS)和整体径向应变(GRS)。收集基线临床因素,包括性别、年龄和传统心血管危险因素,以及低密度脂蛋白胆固醇、高密度脂蛋白胆固醇(HDL-C)、甘油三酯(TG)和血清肌酐水平。采用多变量logistic回归分析确定脑脊液的独立预测因子,并建立脑脊液的联合预测模型。通过受试者工作特征(ROC)曲线评价参数的预测准确性。结果:共纳入146例接受CAG和CMR的患者,并根据CTFC分为CSF组(n=73, 78.1%男性,年龄49.44±9.59岁)和对照组(n=73, 57.5%男性,年龄47.32±13.57岁)。与对照组相比,脑脊液患者更有可能有较高的BMI、高尿酸血症、外周动脉疾病和吸烟习惯,以及较低的HDL-C水平和较高的tg。与对照组相比,CSF患者GLS(-12.09%±2.69% vs -14.38%±2.36%)、GCS(-18.70%±3.24% vs -19.80%±2.21%)和HDL-C (0.783 vs 0.654, P=0.003)分别受损(P值分别为15.25%±8.50%、0.616、0.742,P=0.130)。结论:CMR引起的HDL-C降低、PI降低和GLS可作为脑脊液的预测因子。需要更多的多中心随机对照试验来验证这些发现。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


