Rui Wang, Shuo Leng, Han Xu, Zhiming Tian, Shujuan Xu, Yi Zhang
{"title":"Dual-volume reconstruction technology in the detection and classification of recurrent aneurysms following intracranial aneurysm embolization.","authors":"Rui Wang, Shuo Leng, Han Xu, Zhiming Tian, Shujuan Xu, Yi Zhang","doi":"10.21037/qims-2025-303","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Accurate detection of recurrent intracranial aneurysms (ICAs) after embolization is critical for guiding clinical management and preventing re-rupture. Although two-dimensional digital subtraction angiography (2D-DSA) remains the gold standard, its invasive nature limits routine use. Non-invasive imaging modalities such as computed tomography angiography (CTA) and magnetic resonance angiography (MRA) have limitations in detecting small or morphologically complex recurrent aneurysms. This study aimed to evaluate the diagnostic performance of dual-volume reconstruction technology (DVRT) in comparison to CTA and MRA for detecting recurrent ICA and to explore the correlation between aneurysm imaging characteristics and clinical outcomes.</p><p><strong>Methods: </strong>This retrospective study included 152 patients who underwent ICA embolization and subsequent follow-up imaging with CTA, MRA, and DVRT. All patients received standardized pre-procedural imaging (CTA, MRA, and DVRT) within 48 hours before intervention to document baseline aneurysm characteristics including size, morphology, and location. Postoperative surveillance was systematically performed using triple-modality imaging (CTA, MRA, and DVRT) at 3- and 12-month intervals to monitor treatment efficacy and detect potential recurrence. For the classification of recurrent aneurysms, post-embolization imaging attributes (size, morphology, location) were compared to pre-embolization baseline data to confirm recurrence. Multivariable logistic regression analysis was applied to pre-embolization characteristics to predict recurrence risk. Visualization techniques, including heatmaps and forest plots, were used to illustrate comparative detection performance.</p><p><strong>Results: </strong>DVRT demonstrated higher detection rates for recurrent aneurysms (94.4%, 17/18) compared to CTA (77.8%, 14/18) and MRA (50.0%, 9/18) (P<0.001), with notable performance for small aneurysms (<5 mm: 80.0% <i>vs.</i> 60.0% <i>vs.</i> 40.0%; P=0.317) and medium aneurysms (5-10 mm: 100.0% <i>vs.</i> 88.9% <i>vs.</i> 55.6%; P=0.012). Morphological analysis showed that DVRT had high detection rates for saccular (100.0% <i>vs.</i> 88.9% <i>vs.</i> 66.7%; P=0.039) and lobulated aneurysms (100.0% <i>vs.</i> 75.0% <i>vs.</i> 50.0%; P=0.250), while maintaining detection rates of 92.3% for anterior circulation (<i>vs.</i> 76.9% <i>vs.</i> 46.2%; P=0.008) and 100.0% for posterior circulation aneurysms (<i>vs.</i> 80.0% <i>vs.</i> 60.0%; P=0.200) compared to CTA and MRA, respectively. Multivariable analysis identified size >10 mm [odds ratio (OR) =2.51, 95% confidence interval (CI): 1.83-3.51, P=0.030], irregular morphology (OR =3.02, 95% CI: 2.15-4.43, P=0.003), and posterior location (OR =2.07, 95% CI: 1.43-2.91, P<0.001) as independent predictors of recurrence. Heatmap and forest plot analyses highlighted DVRT's improved diagnostic consistency and narrower CIs across different aneurysm subtypes.</p><p><strong>Conclusions: </strong>DVRT offers superior diagnostic accuracy in detecting recurrent ICA following embolization compared to CTA and MRA, particularly for small, irregularly shaped, and posterior circulation aneurysms. Its advanced imaging capabilities support early detection of recurrence, informed risk stratification, and optimized clinical management strategies. Integration of DVRT into routine postoperative surveillance may improve long-term outcomes for patients with ICA.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 9","pages":"8008-8022"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397631/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-2025-303","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Accurate detection of recurrent intracranial aneurysms (ICAs) after embolization is critical for guiding clinical management and preventing re-rupture. Although two-dimensional digital subtraction angiography (2D-DSA) remains the gold standard, its invasive nature limits routine use. Non-invasive imaging modalities such as computed tomography angiography (CTA) and magnetic resonance angiography (MRA) have limitations in detecting small or morphologically complex recurrent aneurysms. This study aimed to evaluate the diagnostic performance of dual-volume reconstruction technology (DVRT) in comparison to CTA and MRA for detecting recurrent ICA and to explore the correlation between aneurysm imaging characteristics and clinical outcomes.
Methods: This retrospective study included 152 patients who underwent ICA embolization and subsequent follow-up imaging with CTA, MRA, and DVRT. All patients received standardized pre-procedural imaging (CTA, MRA, and DVRT) within 48 hours before intervention to document baseline aneurysm characteristics including size, morphology, and location. Postoperative surveillance was systematically performed using triple-modality imaging (CTA, MRA, and DVRT) at 3- and 12-month intervals to monitor treatment efficacy and detect potential recurrence. For the classification of recurrent aneurysms, post-embolization imaging attributes (size, morphology, location) were compared to pre-embolization baseline data to confirm recurrence. Multivariable logistic regression analysis was applied to pre-embolization characteristics to predict recurrence risk. Visualization techniques, including heatmaps and forest plots, were used to illustrate comparative detection performance.
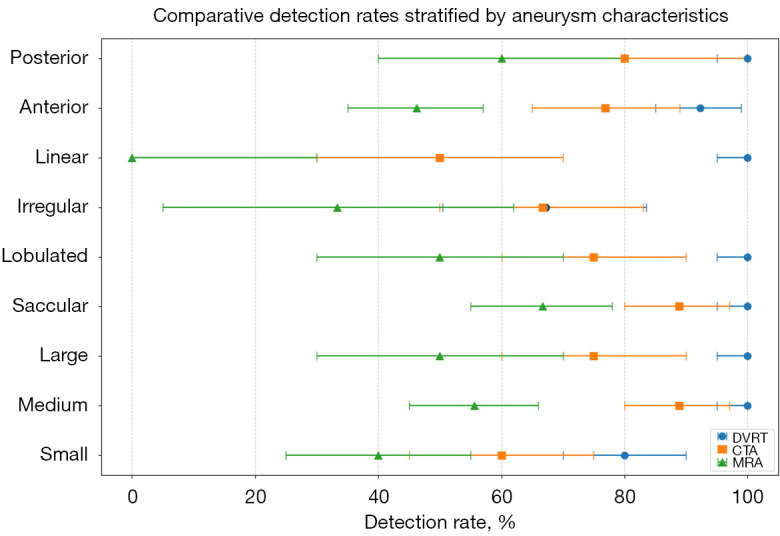
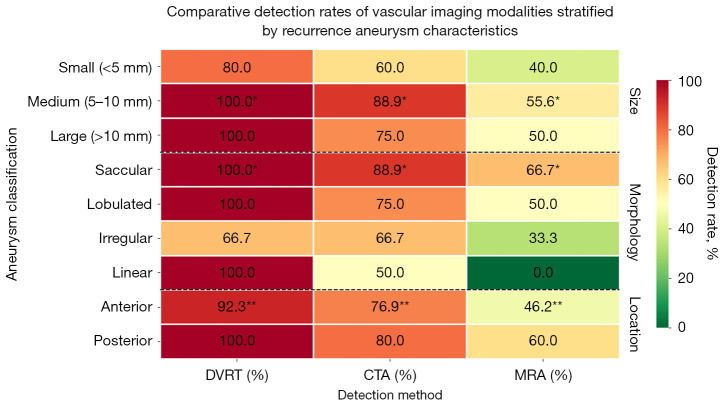
Results: DVRT demonstrated higher detection rates for recurrent aneurysms (94.4%, 17/18) compared to CTA (77.8%, 14/18) and MRA (50.0%, 9/18) (P<0.001), with notable performance for small aneurysms (<5 mm: 80.0% vs. 60.0% vs. 40.0%; P=0.317) and medium aneurysms (5-10 mm: 100.0% vs. 88.9% vs. 55.6%; P=0.012). Morphological analysis showed that DVRT had high detection rates for saccular (100.0% vs. 88.9% vs. 66.7%; P=0.039) and lobulated aneurysms (100.0% vs. 75.0% vs. 50.0%; P=0.250), while maintaining detection rates of 92.3% for anterior circulation (vs. 76.9% vs. 46.2%; P=0.008) and 100.0% for posterior circulation aneurysms (vs. 80.0% vs. 60.0%; P=0.200) compared to CTA and MRA, respectively. Multivariable analysis identified size >10 mm [odds ratio (OR) =2.51, 95% confidence interval (CI): 1.83-3.51, P=0.030], irregular morphology (OR =3.02, 95% CI: 2.15-4.43, P=0.003), and posterior location (OR =2.07, 95% CI: 1.43-2.91, P<0.001) as independent predictors of recurrence. Heatmap and forest plot analyses highlighted DVRT's improved diagnostic consistency and narrower CIs across different aneurysm subtypes.
Conclusions: DVRT offers superior diagnostic accuracy in detecting recurrent ICA following embolization compared to CTA and MRA, particularly for small, irregularly shaped, and posterior circulation aneurysms. Its advanced imaging capabilities support early detection of recurrence, informed risk stratification, and optimized clinical management strategies. Integration of DVRT into routine postoperative surveillance may improve long-term outcomes for patients with ICA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


