Simona Kurková, Martin Kynčl, Ibrahim Ibrahim, Hynek Lachman, Kristina Sakmárová, Stanislav Machač
{"title":"Exploring non-invasive diagnostic tools for deep gluteal syndrome: a multimodal approach integrating clinical and imaging techniques.","authors":"Simona Kurková, Martin Kynčl, Ibrahim Ibrahim, Hynek Lachman, Kristina Sakmárová, Stanislav Machač","doi":"10.21037/qims-2025-241","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Deep gluteal syndrome (DGS) involves extrapelvic entrapment or irritation of the sciatic nerve (SN) within the deep gluteal space, often mimicking S1 radicular syndrome. Accurate differentiation between DGS and true nerve root pathology is essential for effective treatment. This study aimed to distinguish DGS from nerve root affections and identify the causes of symptoms in individuals with suspected DGS using a comprehensive multi-modal evaluation, including advanced diagnostic techniques.</p><p><strong>Methods: </strong>Nineteen subjects (13 females, 6 males, mean age of 36.8±10.9 years, range 23-65 years) with unilateral gluteal pain radiating to the S1 dermatome for at least three months and symptoms exacerbated by prolonged sitting were evaluated. All underwent 3T magnetic resonance imaging (MRI) (Siemens MAGNETOM VIDA) for standard spine and pelvis imaging, diffusion tensor imaging (DTI) of the lumbosacral plexus (LSP) and SN, electromyography (EMG) of the H-reflex circuit with positional maneuvers, and clinical tests targeting DGS.</p><p><strong>Results: </strong>Nerve root contact was demonstrated in only two subjects on the pathology side. Morphological findings on standard MRI with the potential to cause DGS symptoms were inconsistent. Surprisingly, narrowing between the ischium and lesser trochanter of the femur was found in 42% on the symptomatic side. Statistically significant higher mean diffusivity (MD) (P=0.023), radial diffusivity (RD) (P=0.038), and axial diffusivity (AD) (P=0.026) values were observed on the symptomatic side of the SN, indicating edema and microstructural changes. No significant differences were noted in fractional anisotropy (FA) (P=0.913) and normalized quantitative anisotropy (NQA) values (P=0.778). No changes in diffusivity were observed at the LSP level. Twelve subjects (63%) showed increased latency (>1.2 ms) or complete disappearance of the H-reflex when using modified muscle position/activation on the symptomatic side. Clinical tests showed inconclusive results.</p><p><strong>Conclusions: </strong>Advanced diagnostic tools such as DTI and EMG combined with positional maneuvers can help identify DGS when standard imaging and clinical tests are inconclusive. Elevated diffusivity values in the symptomatic SN suggest possible edema and structural changes, supporting the utility of a multimodal approach for accurate diagnosis and treatment of DGS.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 9","pages":"8409-8422"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397617/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-2025-241","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Deep gluteal syndrome (DGS) involves extrapelvic entrapment or irritation of the sciatic nerve (SN) within the deep gluteal space, often mimicking S1 radicular syndrome. Accurate differentiation between DGS and true nerve root pathology is essential for effective treatment. This study aimed to distinguish DGS from nerve root affections and identify the causes of symptoms in individuals with suspected DGS using a comprehensive multi-modal evaluation, including advanced diagnostic techniques.
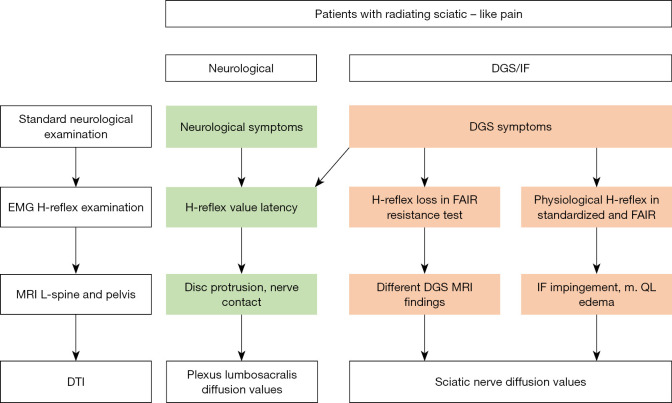
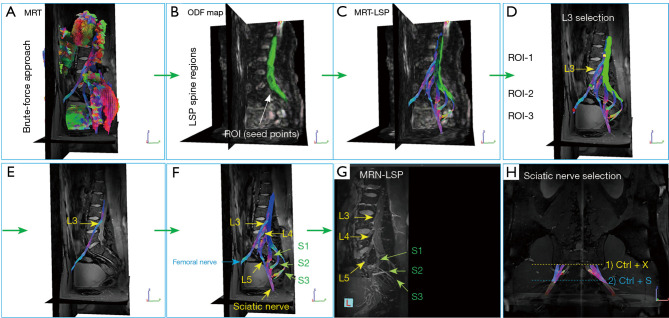
Methods: Nineteen subjects (13 females, 6 males, mean age of 36.8±10.9 years, range 23-65 years) with unilateral gluteal pain radiating to the S1 dermatome for at least three months and symptoms exacerbated by prolonged sitting were evaluated. All underwent 3T magnetic resonance imaging (MRI) (Siemens MAGNETOM VIDA) for standard spine and pelvis imaging, diffusion tensor imaging (DTI) of the lumbosacral plexus (LSP) and SN, electromyography (EMG) of the H-reflex circuit with positional maneuvers, and clinical tests targeting DGS.
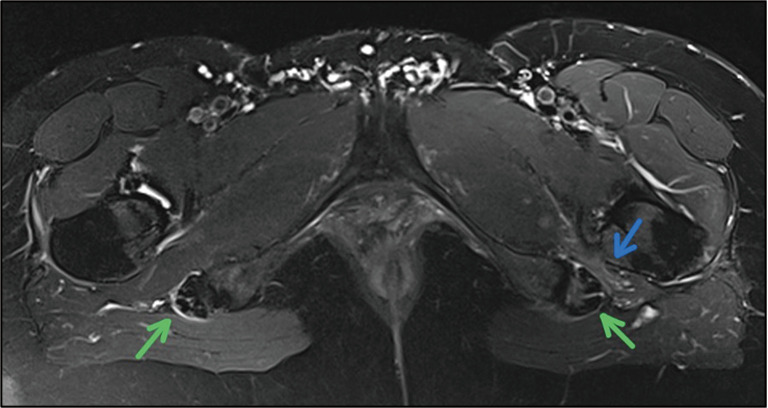
Results: Nerve root contact was demonstrated in only two subjects on the pathology side. Morphological findings on standard MRI with the potential to cause DGS symptoms were inconsistent. Surprisingly, narrowing between the ischium and lesser trochanter of the femur was found in 42% on the symptomatic side. Statistically significant higher mean diffusivity (MD) (P=0.023), radial diffusivity (RD) (P=0.038), and axial diffusivity (AD) (P=0.026) values were observed on the symptomatic side of the SN, indicating edema and microstructural changes. No significant differences were noted in fractional anisotropy (FA) (P=0.913) and normalized quantitative anisotropy (NQA) values (P=0.778). No changes in diffusivity were observed at the LSP level. Twelve subjects (63%) showed increased latency (>1.2 ms) or complete disappearance of the H-reflex when using modified muscle position/activation on the symptomatic side. Clinical tests showed inconclusive results.
Conclusions: Advanced diagnostic tools such as DTI and EMG combined with positional maneuvers can help identify DGS when standard imaging and clinical tests are inconclusive. Elevated diffusivity values in the symptomatic SN suggest possible edema and structural changes, supporting the utility of a multimodal approach for accurate diagnosis and treatment of DGS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


