{"title":"Algorithms to Improve Fairness in Medicare Risk Adjustment.","authors":"Marissa B Reitsma, Thomas G McGuire, Sherri Rose","doi":"10.1001/jamahealthforum.2025.2640","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Payment system design creates incentives that affect health care spending, access, and outcomes. With Medicare Advantage accounting for more than half of Medicare spending, changes to its risk adjustment algorithm have the potential for broad consequences.</p><p><strong>Objective: </strong>To assess the potential for algorithmic tools to achieve more equitable plan payment for Medicare risk adjustment while maintaining current levels of performance, flexibility, feasibility, transparency, and interpretability.</p><p><strong>Design, setting, and participants: </strong>This diagnostic study included a retrospective analysis of traditional Medicare enrollment and claims data generated between January 1, 2017, and December 31, 2020, from a random 20% sample of non-dual-eligible Medicare beneficiaries with documented residence in the US or Puerto Rico. Race and ethnicity were designated using the Research Triangle Institute enhanced indicator. Diagnoses in claims were mapped to hierarchical condition categories. Algorithms used demographic indicators and hierarchical condition categories from 1 calendar year to predict Medicare spending in the subsequent year. Data analysis was conducted between August 16, 2023, and January 27, 2025.</p><p><strong>Main outcomes and measures: </strong>The main outcome was prospective health care spending by Medicare. Overall performance was measured by payment system fit and mean absolute error. Net compensation was used to assess group-level fairness.</p><p><strong>Results: </strong>The main analysis of Medicare risk adjustment algorithms included 4 398 035 Medicare beneficiaries with a mean (SD) age of 75.2 (7.4) years and mean (SD) annual Medicare spending of $8345 ($18 581); 44% were men; fewer than 1% were American Indian or Alaska Native, 2% were Asian or Other Pacific Islander, 6% were Black, 3% were Hispanic, 86% were non-Hispanic White, and 1% were part of an additional group (termed as other in the Centers for Medicare & Medicaid Services data). Out-of-sample payment system fit for the baseline regression was 12.7%. Constrained regression and postprocessing both achieved fair spending targets while maintaining payment system fit (constrained regression, 12.6%; postprocessing, 12.7%). Whereas postprocessing increased mean payments for beneficiaries in minoritized racial and ethnic groups (American Indian or Alaska Native, Asian or Other Pacific Islander, Black, and Hispanic individuals) only, constrained regression increased mean payments for beneficiaries in minoritized racial and ethnic groups and beneficiaries in other groups residing in counties with greater exposure to socioeconomic factors that can adversely affect health outcomes.</p><p><strong>Conclusions and relevance: </strong>Results of this study suggest that constrained regression and postprocessing can incorporate fairness objectives into the Medicare risk adjustment algorithm with minimal reduction in overall fit. These feasible changes to the Medicare risk adjustment algorithm could be considered by policymakers aiming to address health care disparities through payment system reform.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"6 8","pages":"e252640"},"PeriodicalIF":11.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397885/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2025.2640","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: Payment system design creates incentives that affect health care spending, access, and outcomes. With Medicare Advantage accounting for more than half of Medicare spending, changes to its risk adjustment algorithm have the potential for broad consequences.
Objective: To assess the potential for algorithmic tools to achieve more equitable plan payment for Medicare risk adjustment while maintaining current levels of performance, flexibility, feasibility, transparency, and interpretability.
Design, setting, and participants: This diagnostic study included a retrospective analysis of traditional Medicare enrollment and claims data generated between January 1, 2017, and December 31, 2020, from a random 20% sample of non-dual-eligible Medicare beneficiaries with documented residence in the US or Puerto Rico. Race and ethnicity were designated using the Research Triangle Institute enhanced indicator. Diagnoses in claims were mapped to hierarchical condition categories. Algorithms used demographic indicators and hierarchical condition categories from 1 calendar year to predict Medicare spending in the subsequent year. Data analysis was conducted between August 16, 2023, and January 27, 2025.
Main outcomes and measures: The main outcome was prospective health care spending by Medicare. Overall performance was measured by payment system fit and mean absolute error. Net compensation was used to assess group-level fairness.
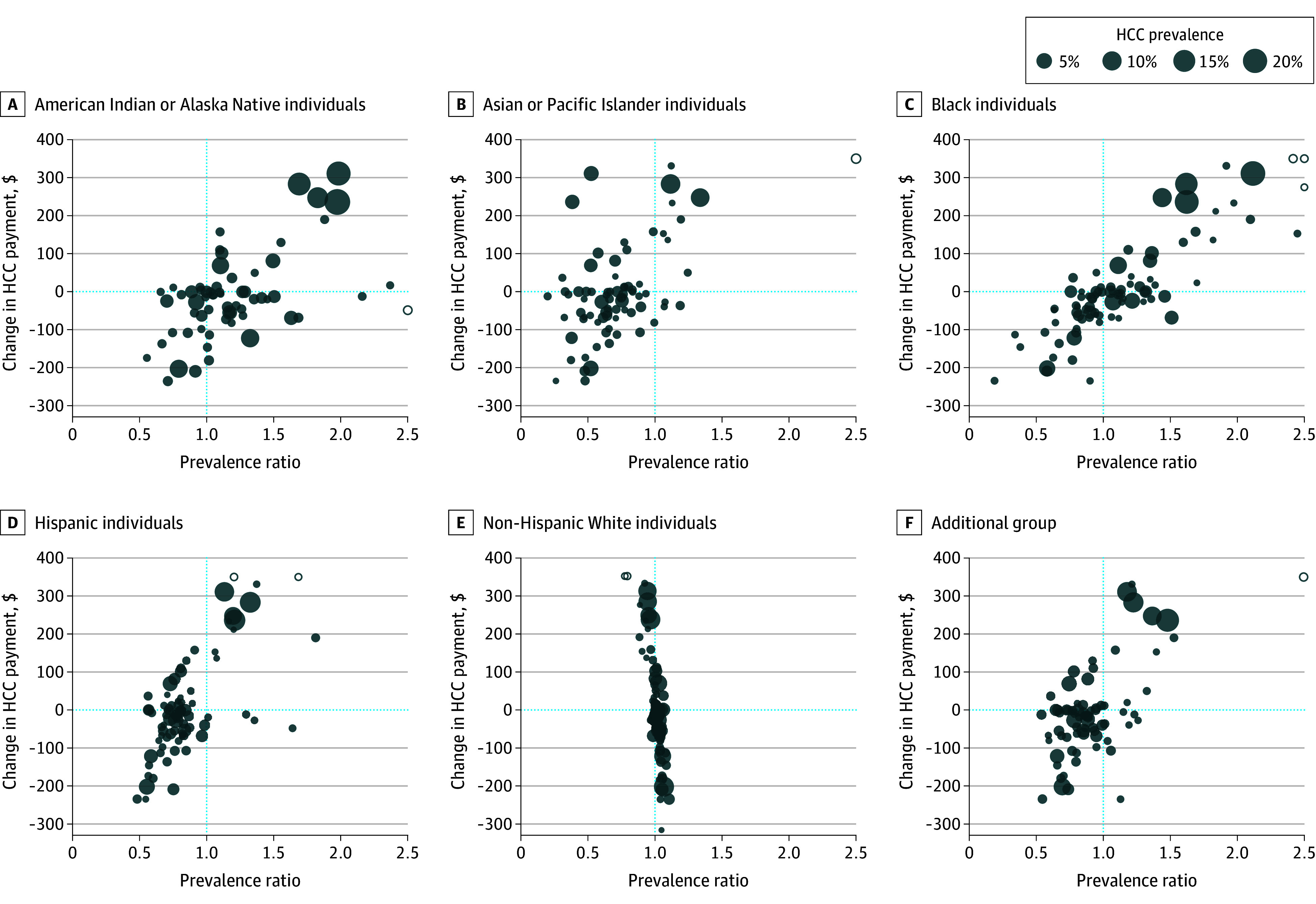
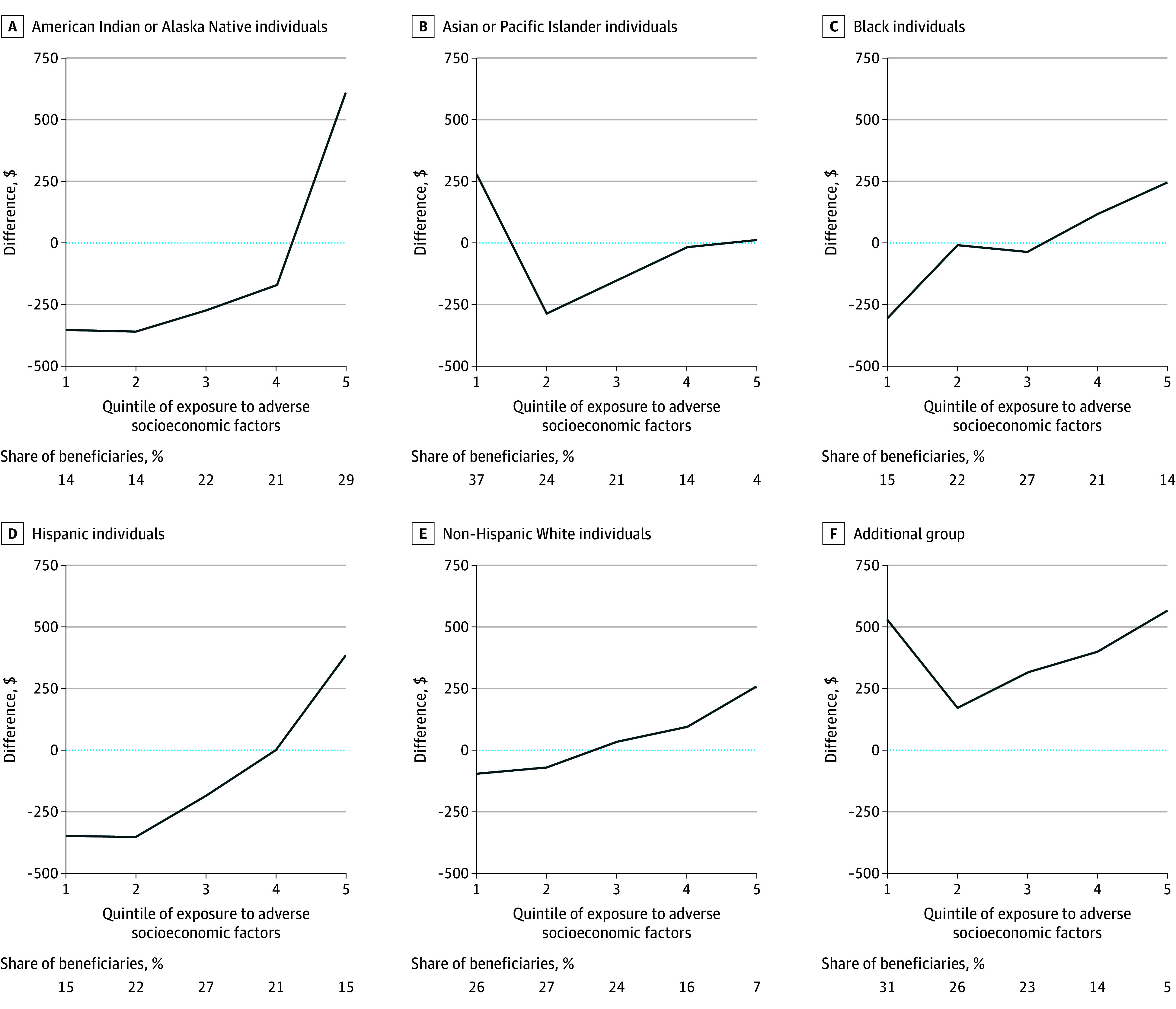
Results: The main analysis of Medicare risk adjustment algorithms included 4 398 035 Medicare beneficiaries with a mean (SD) age of 75.2 (7.4) years and mean (SD) annual Medicare spending of $8345 ($18 581); 44% were men; fewer than 1% were American Indian or Alaska Native, 2% were Asian or Other Pacific Islander, 6% were Black, 3% were Hispanic, 86% were non-Hispanic White, and 1% were part of an additional group (termed as other in the Centers for Medicare & Medicaid Services data). Out-of-sample payment system fit for the baseline regression was 12.7%. Constrained regression and postprocessing both achieved fair spending targets while maintaining payment system fit (constrained regression, 12.6%; postprocessing, 12.7%). Whereas postprocessing increased mean payments for beneficiaries in minoritized racial and ethnic groups (American Indian or Alaska Native, Asian or Other Pacific Islander, Black, and Hispanic individuals) only, constrained regression increased mean payments for beneficiaries in minoritized racial and ethnic groups and beneficiaries in other groups residing in counties with greater exposure to socioeconomic factors that can adversely affect health outcomes.
Conclusions and relevance: Results of this study suggest that constrained regression and postprocessing can incorporate fairness objectives into the Medicare risk adjustment algorithm with minimal reduction in overall fit. These feasible changes to the Medicare risk adjustment algorithm could be considered by policymakers aiming to address health care disparities through payment system reform.
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


