Clinical value of fluorescence laparoscopic surgery on anastomotic leakage prevention in ultra-low rectal cancer: real-world multicenter retrospective evidence with neoadjuvant chemoradiotherapy stratification.
{"title":"Clinical value of fluorescence laparoscopic surgery on anastomotic leakage prevention in ultra-low rectal cancer: real-world multicenter retrospective evidence with neoadjuvant chemoradiotherapy stratification.","authors":"W Qiu, G Hu, K He, S Mei, Z Xing, Y Li, J Tang","doi":"10.1007/s10151-025-03203-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neoadjuvant chemoradiotherapy (nCRT) is key for low rectal cancer but raises the risk of anastomotic leakage (AL). This study examines how fluorescence laparoscopic (FL) surgery reduces AL after intersphincteric resection (ISR), especially in nCRT patients.</p><p><strong>Methods: </strong>This real-world multicenter cohort study included 533 patients undergoing laparoscopic ISR for ultra-low rectal adenocarcinoma from January 2012 to July 2023. Patients were categorized into FL and non-FL groups. Propensity score matching (PSM) was used at a 1:2 ratio to adjust for baseline differences. The primary endpoint was the incidence of AL within 6 months postoperatively. Secondary endpoints included anastomotic site perfusion, intraoperative blood loss, lymph node retrieval, perioperative complications, and postoperative recovery metrics. Subgroup analyses were conducted on the basis of nCRT status.</p><p><strong>Results: </strong>After PSM, 393 patients were analyzed (131 FL versus 262 non-FL). The FL group showed a significantly lower AL incidence (3.1% versus 11.5%, P = 0.005), with fewer severe symptomatic AL cases (0.8% versus 6.1%, P = 0.014). Intraoperative blood loss was reduced (45.2 ± 58.9 mL versus 65.3 ± 73.1 mL, P = 0.004), and lymph node yield was higher (21.2 ± 11.4 versus 16.6 ± 7.3, P < 0.001) in the FL group. Postoperative recovery was accelerated, with earlier return of bowel function and shorter hospital stays (9.5 ± 3.1 versus 10.7 ± 3.8 days, P = 0.012). In subgroup analyses, FL significantly reduced AL rates in patients without nCRT (1.9% versus 7.2%, P = 0.045) and demonstrated a strong trend toward reduction in AL for patients receiving nCRT (13.0% versus 35.9%, P = 0.051). FL also increased the proportion of patients achieving benchmark lymph node retrieval, including those post-nCRT.</p><p><strong>Conclusions: </strong>Fluorescence-guided laparoscopic surgery reduces anastomotic leakage and improves outcomes in low rectal cancer, especially after chemoradiotherapy, by enhancing surgical precision and recovery.</p>","PeriodicalId":51192,"journal":{"name":"Techniques in Coloproctology","volume":"29 1","pages":"165"},"PeriodicalIF":2.9000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12370547/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Techniques in Coloproctology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10151-025-03203-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Neoadjuvant chemoradiotherapy (nCRT) is key for low rectal cancer but raises the risk of anastomotic leakage (AL). This study examines how fluorescence laparoscopic (FL) surgery reduces AL after intersphincteric resection (ISR), especially in nCRT patients.
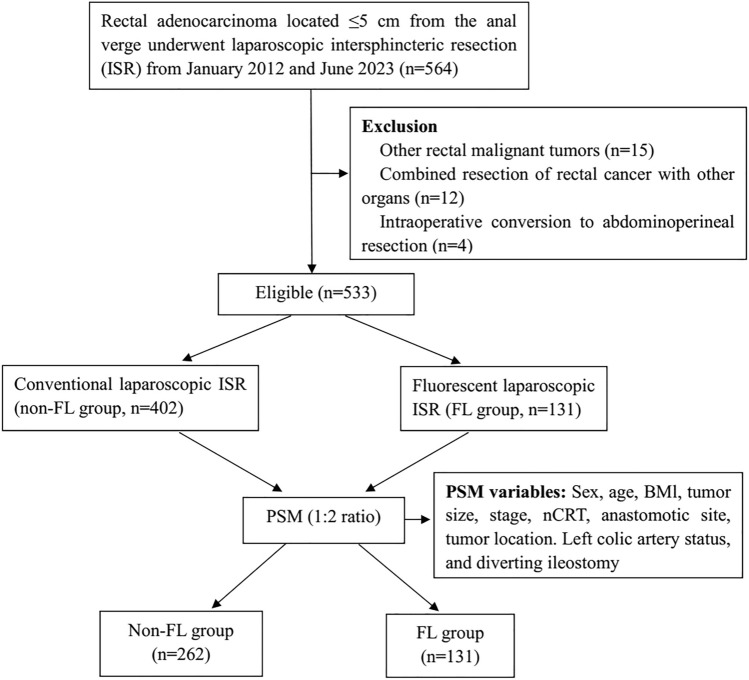
Methods: This real-world multicenter cohort study included 533 patients undergoing laparoscopic ISR for ultra-low rectal adenocarcinoma from January 2012 to July 2023. Patients were categorized into FL and non-FL groups. Propensity score matching (PSM) was used at a 1:2 ratio to adjust for baseline differences. The primary endpoint was the incidence of AL within 6 months postoperatively. Secondary endpoints included anastomotic site perfusion, intraoperative blood loss, lymph node retrieval, perioperative complications, and postoperative recovery metrics. Subgroup analyses were conducted on the basis of nCRT status.
Results: After PSM, 393 patients were analyzed (131 FL versus 262 non-FL). The FL group showed a significantly lower AL incidence (3.1% versus 11.5%, P = 0.005), with fewer severe symptomatic AL cases (0.8% versus 6.1%, P = 0.014). Intraoperative blood loss was reduced (45.2 ± 58.9 mL versus 65.3 ± 73.1 mL, P = 0.004), and lymph node yield was higher (21.2 ± 11.4 versus 16.6 ± 7.3, P < 0.001) in the FL group. Postoperative recovery was accelerated, with earlier return of bowel function and shorter hospital stays (9.5 ± 3.1 versus 10.7 ± 3.8 days, P = 0.012). In subgroup analyses, FL significantly reduced AL rates in patients without nCRT (1.9% versus 7.2%, P = 0.045) and demonstrated a strong trend toward reduction in AL for patients receiving nCRT (13.0% versus 35.9%, P = 0.051). FL also increased the proportion of patients achieving benchmark lymph node retrieval, including those post-nCRT.
Conclusions: Fluorescence-guided laparoscopic surgery reduces anastomotic leakage and improves outcomes in low rectal cancer, especially after chemoradiotherapy, by enhancing surgical precision and recovery.
期刊介绍:
Techniques in Coloproctology is an international journal fully devoted to diagnostic and operative procedures carried out in the management of colorectal diseases. Imaging, clinical physiology, laparoscopy, open abdominal surgery and proctoperineology are the main topics covered by the journal. Reviews, original articles, technical notes and short communications with many detailed illustrations render this publication indispensable for coloproctologists and related specialists. Both surgeons and gastroenterologists are represented on the distinguished Editorial Board, together with pathologists, radiologists and basic scientists from all over the world. The journal is strongly recommended to those who wish to be updated on recent developments in the field, and improve the standards of their work.
Manuscripts submitted for publication must contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1965 Declaration of Helsinki. It should also be stated clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study should be omitted. Reports of animal experiments must state that the Principles of Laboratory Animal Care (NIH publication no. 86-23 revised 1985) were followed as were applicable national laws (e.g. the current version of the German Law on the Protection of Animals). The Editor-in-Chief reserves the right to reject manuscripts that do not comply with the above-mentioned requirements. Authors will be held responsible for false statements or for failure to fulfill such requirements.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


