Continuous versus intermittent noninvasive blood pressure measurement in patients with shock in prehospital emergency medicine - a single-center prospective pilot trial.
Stephan Katzenschlager, Raphael Heck, Nikolai Kaltschmidt, Frank Weilbacher, Markus A Weigand, Erik Popp, Maximilian Dietrich
{"title":"Continuous versus intermittent noninvasive blood pressure measurement in patients with shock in prehospital emergency medicine - a single-center prospective pilot trial.","authors":"Stephan Katzenschlager, Raphael Heck, Nikolai Kaltschmidt, Frank Weilbacher, Markus A Weigand, Erik Popp, Maximilian Dietrich","doi":"10.1186/s13049-025-01457-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Shock is a critical and potentially life-threatening clinical state characterized by circulatory insufficiency and impaired micro- and macrocirculation. Rapid detection and initiation of therapy are essential for patient outcomes. In prehospital emergency medicine, assessment tools are limited, and intermittent noninvasive blood pressure (iNIBP) monitoring is the current standard of care. Recent findings suggest that this method may miss episodes of relevant hypotension. Continuous noninvasive blood pressure (cNIBP) and tissue oxygenation (StO<sub>2</sub>) measurements could improve the time to detection of shock.</p><p><strong>Methods: </strong>This single-center prospective pilot trial compared a cNIBP system with standard iNIBP measurements in physician-staffed prehospital care. The study was conducted in the Rhine-Neckar region between May and December 2023. The Edwards HemoSphere system, including ClearSight for cNIBP and ForeSight for StO<sub>2</sub>, was used in conjunction with standard monitoring. Adults with shock were eligible for inclusion. Primary endpoint was the agreement between cNIBP and iNIBP; secondary endpoints included unrecognized hypotension (MAP < 60 mmHg) and comparison between cNIBP/iNIBP and StO<sub>2</sub>. Bland-Altman analysis quantified bias and limits of agreement (LoA).</p><p><strong>Results: </strong>In total, 25 patients were included, resulting in 100 simultaneous measurements. iNIBP readings exceeded cNIBP measurements of mean arterial pressure (MAP) by 10.77 mmHg (p < 0.01). There were further significant differences for systolic and diastolic blood pressure, with higher values for iNIBP measurements. Bland-Altman analysis demonstrated systemic bias (MAP bias - 10.25) with wide LoA (-43.52 to 22.21), indicating poor interchangeability. In three out of 25 cases, standard intermittent blood pressure measurements failed to detect hypotension, although cNIBP showed MAP values below 60 mmHg.</p><p><strong>Conclusion: </strong>Our pilot data show cNIBP and iNIBP values differ significantly, with clinical implications, potentially improving hemodynamic instability detection. However, as this is preliminary, more research on system reliability and benefits of enhanced monitoring is needed.</p><p><strong>Trial registration: </strong>German Clinical Trials Registry (DRKS ID DRKS00031867) on 22.05.2023.</p>","PeriodicalId":49292,"journal":{"name":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","volume":"33 1","pages":"143"},"PeriodicalIF":3.1000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12369113/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-025-01457-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Shock is a critical and potentially life-threatening clinical state characterized by circulatory insufficiency and impaired micro- and macrocirculation. Rapid detection and initiation of therapy are essential for patient outcomes. In prehospital emergency medicine, assessment tools are limited, and intermittent noninvasive blood pressure (iNIBP) monitoring is the current standard of care. Recent findings suggest that this method may miss episodes of relevant hypotension. Continuous noninvasive blood pressure (cNIBP) and tissue oxygenation (StO2) measurements could improve the time to detection of shock.
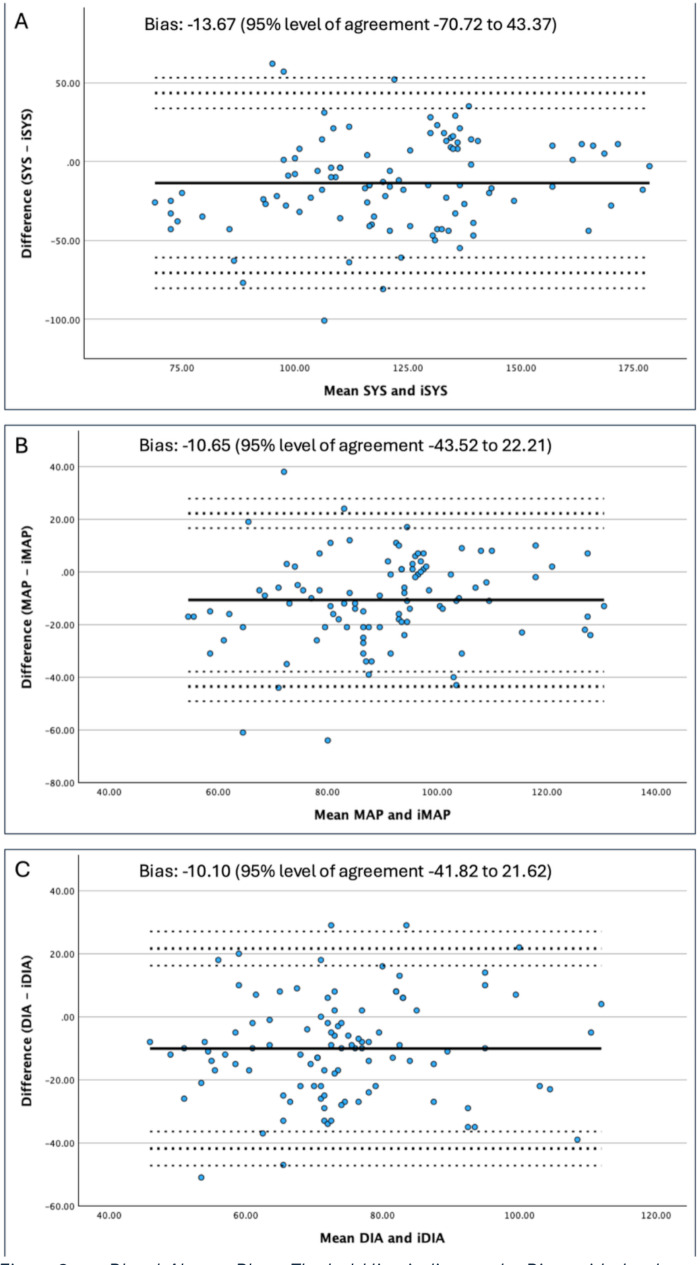
Methods: This single-center prospective pilot trial compared a cNIBP system with standard iNIBP measurements in physician-staffed prehospital care. The study was conducted in the Rhine-Neckar region between May and December 2023. The Edwards HemoSphere system, including ClearSight for cNIBP and ForeSight for StO2, was used in conjunction with standard monitoring. Adults with shock were eligible for inclusion. Primary endpoint was the agreement between cNIBP and iNIBP; secondary endpoints included unrecognized hypotension (MAP < 60 mmHg) and comparison between cNIBP/iNIBP and StO2. Bland-Altman analysis quantified bias and limits of agreement (LoA).
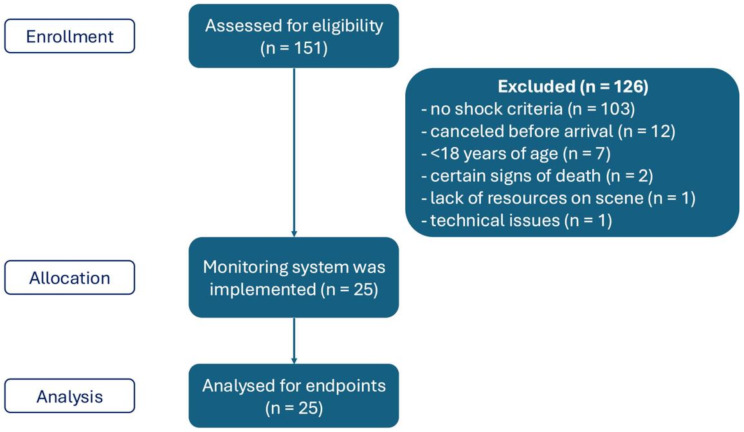
Results: In total, 25 patients were included, resulting in 100 simultaneous measurements. iNIBP readings exceeded cNIBP measurements of mean arterial pressure (MAP) by 10.77 mmHg (p < 0.01). There were further significant differences for systolic and diastolic blood pressure, with higher values for iNIBP measurements. Bland-Altman analysis demonstrated systemic bias (MAP bias - 10.25) with wide LoA (-43.52 to 22.21), indicating poor interchangeability. In three out of 25 cases, standard intermittent blood pressure measurements failed to detect hypotension, although cNIBP showed MAP values below 60 mmHg.
Conclusion: Our pilot data show cNIBP and iNIBP values differ significantly, with clinical implications, potentially improving hemodynamic instability detection. However, as this is preliminary, more research on system reliability and benefits of enhanced monitoring is needed.
Trial registration: German Clinical Trials Registry (DRKS ID DRKS00031867) on 22.05.2023.
背景:休克是一种以循环功能不全、微循环和大循环受损为特征的严重的、可能危及生命的临床状态。快速发现和开始治疗对患者的预后至关重要。在院前急诊医学中,评估工具是有限的,间歇性无创血压(iNIBP)监测是目前的标准护理。最近的研究结果表明,这种方法可能会遗漏相关的低血压发作。连续无创血压(cNIBP)和组织氧合(StO2)测量可缩短休克检测时间。方法:本单中心前瞻性试点试验比较了cNIBP系统与医院前医护人员配备的标准iNIBP测量。这项研究于2023年5月至12月在莱茵-内卡地区进行。爱德华兹血球系统,包括用于cNIBP的ClearSight和用于StO2的ForeSight,与标准监测一起使用。有休克的成年人符合入选条件。主要终点是cNIBP和iNIBP之间的协议;次要终点包括无法识别的低血压(MAP 2)。Bland-Altman分析量化了偏差和一致限度(LoA)。结果:共纳入25例患者,同时测量100次。结论:我们的试点数据显示,cNIBP和iNIBP值有显著差异,具有临床意义,可能改善血流动力学不稳定的检测。然而,由于这是初步的,需要对系统可靠性和增强监测的好处进行更多的研究。试验注册:德国临床试验注册中心(DRKS ID DRKS00031867)于2023年5月22日注册。
期刊介绍:
The primary topics of interest in Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (SJTREM) are the pre-hospital and early in-hospital diagnostic and therapeutic aspects of emergency medicine, trauma, and resuscitation. Contributions focusing on dispatch, major incidents, etiology, pathophysiology, rehabilitation, epidemiology, prevention, education, training, implementation, work environment, as well as ethical and socio-economic aspects may also be assessed for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


