Guoqing Zhang, Jia Jiao, Long Qiu, Zheng Ding, Jia Zhao, Xue Pan, Xiangnan Li
{"title":"Rare complications after esophagectomy: incidence, clinical features, risk factors, management, and prevention.","authors":"Guoqing Zhang, Jia Jiao, Long Qiu, Zheng Ding, Jia Zhao, Xue Pan, Xiangnan Li","doi":"10.1177/17562848251366238","DOIUrl":null,"url":null,"abstract":"<p><p>In recent years, common postoperative complications after esophagectomy have received increasing attention. However, the attention paid to rare complications, which often lead to serious consequences if they are not diagnosed in a timely manner, has not been sufficient. In this article, we present both the clinical and imaging features of rare complications following esophagectomy and strategies for their prevention and management. These rare complications are classified into four groups: esophageal substitute-related complications, thoracic duct-related complications, hernia-related complications, and transmural Hem-o-lok clip migration. Esophageal substitute-related complications include redundant conduits and conduit necrosis. We further classify redundant conduits as length-redundant conduits, width-redundant conduits, or a combination of both redundancies. Thoracic duct-related complications include refractory chylothorax and chylomediastinum. Refractory chylothorax is chylothorax refractory to well-established medical, interventional, and even surgical strategies, whereas chylomediastinum is a rare condition characterized by the accumulation of chyle in the mediastinum. Hernia-related complications are subclassified as hiatal hernias, retrocardiac lung hernias, intercostal lung hernias, trocar-site hernias, hernias internal to the retrosternal space or pericardium, and mesenteric defects. Transmural Hem-o-lok clip migration includes penetration of the trachea, conduit, or both. Thoracic surgeons should familiarize themselves with the rare complications of esophagectomy, most of which are serious conditions that require early and accurate diagnosis for proper management. The choice of intervention for rare complications depends on factors such as the patient's general condition, the specific type of complication, the complication severity, the reconstruction route, the available medical resources, and the surgeon's preference. To minimize the risk of these complications, esophagectomy and prevention methods need to be standardized.</p>","PeriodicalId":48770,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"18 ","pages":"17562848251366238"},"PeriodicalIF":3.4000,"publicationDate":"2025-08-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12365439/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848251366238","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
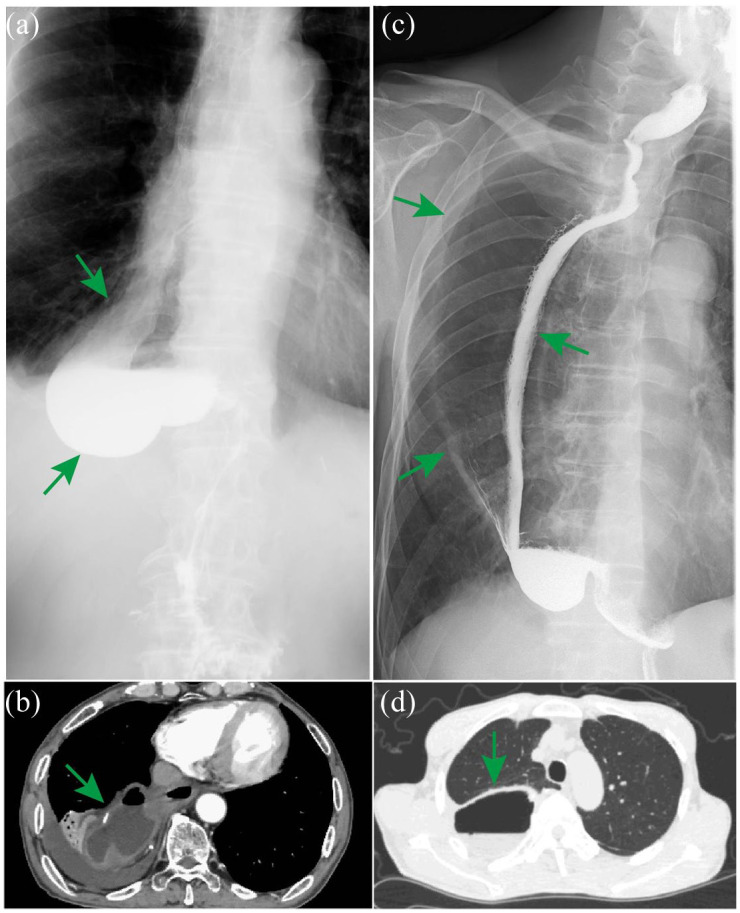
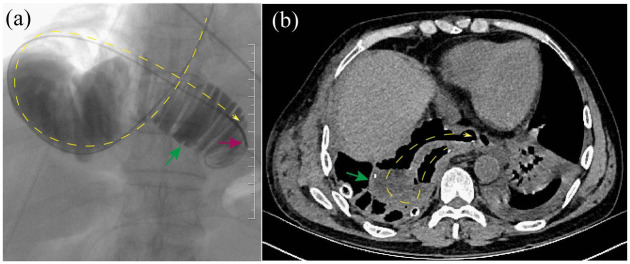
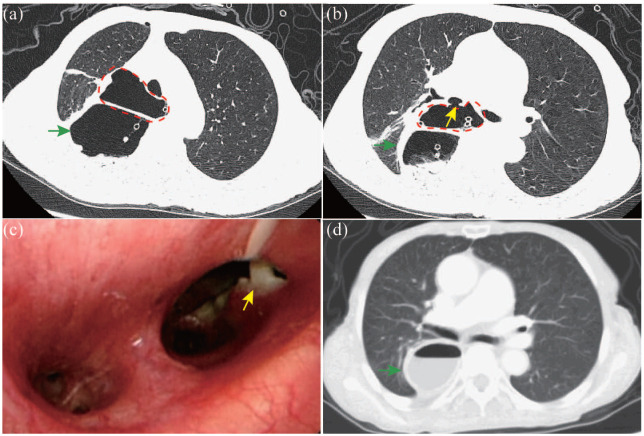
In recent years, common postoperative complications after esophagectomy have received increasing attention. However, the attention paid to rare complications, which often lead to serious consequences if they are not diagnosed in a timely manner, has not been sufficient. In this article, we present both the clinical and imaging features of rare complications following esophagectomy and strategies for their prevention and management. These rare complications are classified into four groups: esophageal substitute-related complications, thoracic duct-related complications, hernia-related complications, and transmural Hem-o-lok clip migration. Esophageal substitute-related complications include redundant conduits and conduit necrosis. We further classify redundant conduits as length-redundant conduits, width-redundant conduits, or a combination of both redundancies. Thoracic duct-related complications include refractory chylothorax and chylomediastinum. Refractory chylothorax is chylothorax refractory to well-established medical, interventional, and even surgical strategies, whereas chylomediastinum is a rare condition characterized by the accumulation of chyle in the mediastinum. Hernia-related complications are subclassified as hiatal hernias, retrocardiac lung hernias, intercostal lung hernias, trocar-site hernias, hernias internal to the retrosternal space or pericardium, and mesenteric defects. Transmural Hem-o-lok clip migration includes penetration of the trachea, conduit, or both. Thoracic surgeons should familiarize themselves with the rare complications of esophagectomy, most of which are serious conditions that require early and accurate diagnosis for proper management. The choice of intervention for rare complications depends on factors such as the patient's general condition, the specific type of complication, the complication severity, the reconstruction route, the available medical resources, and the surgeon's preference. To minimize the risk of these complications, esophagectomy and prevention methods need to be standardized.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


