{"title":"The impact of shortening shifts of physicians during their residency on patients and physicians : A systematic review and meta-analysis.","authors":"Vered Daitch, Itamar Poran, Leonard Leibovici","doi":"10.1186/s13584-025-00715-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prolonged shifts in residency contribute to physician fatigue, cognitive decline, and increased medical errors. This systematic review and meta-analysis evaluate how reducing shift length affects patient-physician safety, physician well-being, and residency training, addressing the ongoing challenge of balancing resident welfare, patient outcomes, and educational standards across varied implementation settings.</p><p><strong>Methods: </strong>A comprehensive search of PubMed, EMBASE, The Cochrane Library, Google Scholar, and opengrey.eu was performed from database inception to January 2024. Eligible studies assessed the effects of duty hour limitations (≤ 24 h) on clinical, educational, or systemic outcomes. Both randomized controlled trials and observational studies were included. Meta-analyses used random-effects models. Risk of bias was assessed with RoB 2.0 and ROBINS-I tools. Subgroup analyses were performed by specialty, shift duration, and publication period. Sensitivity analyses excluded studies with extended timeframes.</p><p><strong>Results: </strong>A total of 108 studies (8 RCTs, 100 observational) were included. Shift shortening was associated with improved resident well-being, including reduced fatigue and work-life balance. Patient safety remained stable, with a significant reduction in 30-day mortality for shifts ≤ 16 h (pooled OR 0.84, 95% CI 0.79-0.89). No significant effect on complications or adverse events was observed. Operative experience showed mixed results, with a non-significant reduction in case volume (pooled std. mean difference 0.65, 95% CI -0.04 to 1.34, P = 0.07), while test scores exhibited minimal changes. Effect directions remained consistent across publication periods. High heterogeneity and risk of bias were observed across most included studies.</p><p><strong>Conclusions: </strong>Shortening shifts to 24 h or less appears to improve residents' satisfaction and work-life balance while maintaining patient safety outcomes. Educational outcomes were mixed; operative experience was preserved in some settings, while effects on non-surgical training remain less clear. These findings underscore the importance of tailoring reforms to specialty needs and training contexts. Future research should examine unstudied outcomes, such as residency attrition or shifts to less demanding specializations, and system-wide implementation costs. A stepped wedge cluster randomized trial is recommended for future policy evaluations.</p><p><strong>Systematic review registration: </strong>PROSPERO CRD42023390197.</p>","PeriodicalId":46694,"journal":{"name":"Israel Journal of Health Policy Research","volume":"14 1","pages":"53"},"PeriodicalIF":2.2000,"publicationDate":"2025-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406601/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Israel Journal of Health Policy Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13584-025-00715-2","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Prolonged shifts in residency contribute to physician fatigue, cognitive decline, and increased medical errors. This systematic review and meta-analysis evaluate how reducing shift length affects patient-physician safety, physician well-being, and residency training, addressing the ongoing challenge of balancing resident welfare, patient outcomes, and educational standards across varied implementation settings.
Methods: A comprehensive search of PubMed, EMBASE, The Cochrane Library, Google Scholar, and opengrey.eu was performed from database inception to January 2024. Eligible studies assessed the effects of duty hour limitations (≤ 24 h) on clinical, educational, or systemic outcomes. Both randomized controlled trials and observational studies were included. Meta-analyses used random-effects models. Risk of bias was assessed with RoB 2.0 and ROBINS-I tools. Subgroup analyses were performed by specialty, shift duration, and publication period. Sensitivity analyses excluded studies with extended timeframes.
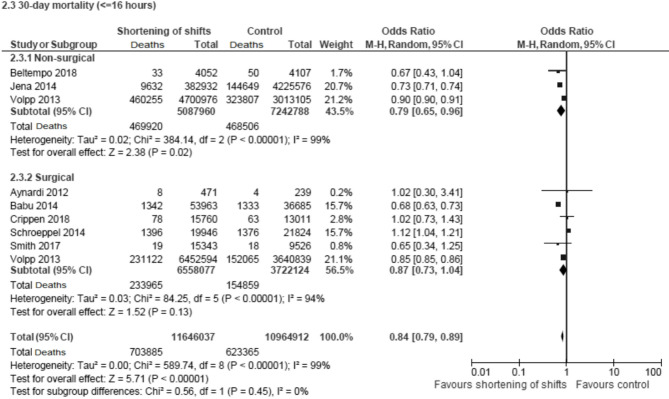
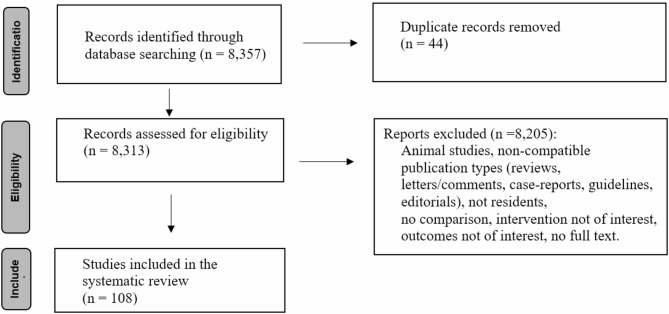
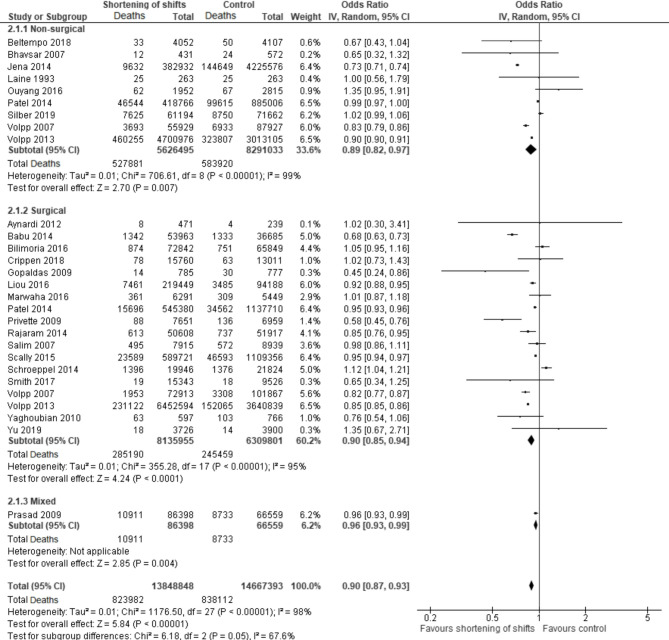
Results: A total of 108 studies (8 RCTs, 100 observational) were included. Shift shortening was associated with improved resident well-being, including reduced fatigue and work-life balance. Patient safety remained stable, with a significant reduction in 30-day mortality for shifts ≤ 16 h (pooled OR 0.84, 95% CI 0.79-0.89). No significant effect on complications or adverse events was observed. Operative experience showed mixed results, with a non-significant reduction in case volume (pooled std. mean difference 0.65, 95% CI -0.04 to 1.34, P = 0.07), while test scores exhibited minimal changes. Effect directions remained consistent across publication periods. High heterogeneity and risk of bias were observed across most included studies.
Conclusions: Shortening shifts to 24 h or less appears to improve residents' satisfaction and work-life balance while maintaining patient safety outcomes. Educational outcomes were mixed; operative experience was preserved in some settings, while effects on non-surgical training remain less clear. These findings underscore the importance of tailoring reforms to specialty needs and training contexts. Future research should examine unstudied outcomes, such as residency attrition or shifts to less demanding specializations, and system-wide implementation costs. A stepped wedge cluster randomized trial is recommended for future policy evaluations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


