{"title":"Survival Predictors and Clinical Outcomes in Patients Undergoing Venoarterial ECMO: A 7-Year Retrospective Study.","authors":"Thavat Chanchayanon, Mantana Saetang, Sutthiphat Wangpholpattanasiri, Ratikorn Boonchai, Pongsanae Duangpakdee","doi":"10.1155/ccrp/5588093","DOIUrl":null,"url":null,"abstract":"<p><p><b>Purpose:</b> Venoarterial extracorporeal membrane oxygenation (VA-ECMO) is a life-saving intervention for refractory cardiopulmonary failure. Identifying factors associated with survival is essential for optimizing patient selection and management. In this study, we aimed to identify VA-ECMO survival predictors and evaluate the associated complications, costs, and outcomes. <b>Methods:</b> A retrospective analysis was conducted on data from 123 adult patients who underwent VA-ECMO at the Songklanagarind Hospital between 2017 and 2023. Clinical characteristics, ECMO-related complications, hospital expenses, and survival outcomes were analyzed. Univariate and multivariate logistic regression analyses were used to determine independent predictors of survival. <b>Results:</b> Fifty (40.7%) patients survived until hospital discharge. Compared to central VA-ECMO, peripheral VA-ECMO was significantly associated with improved survival (adjusted OR: 26.44, 95% CI: 1.95-358.7, <i>p</i> = 0.014). Preexisting liver dysfunction (adjusted OR: 0.27, 95% CI: 0.09-0.79, <i>p</i> = 0.016) and renal dysfunction (adjusted OR: 0.29, 95% CI: 0.1-0.85, <i>p</i> = 0.023) were independent mortality predictors. Survival odds were significantly lower in patients with American Society of Anesthesiologists (ASA) Class 5 (adjusted OR: 0.07, 95% CI: 0.01-0.67, <i>p</i> = 0.022). Neurological complications were more common in nonsurvivors than in survivors (41.1% vs. 18%, <i>p</i> = 0.012). Survivors had significantly higher total hospital costs (997,563.5 vs. 696,191 THB, <i>p</i> = 0.004) and longer hospital stays (28.5 vs. 3 days, <i>p</i> < 0.001). The multivariate model demonstrated strong predictive performance, with an area under the curve of 0.85. <b>Conclusions:</b> ECMO cannulation strategy, preexisting liver and renal dysfunction, and ASA classification were key factors associated with survival. Peripheral VA-ECMO was associated with better outcomes, and organ dysfunction significantly increased the mortality risk.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2025 ","pages":"5588093"},"PeriodicalIF":1.8000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12396898/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/ccrp/5588093","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
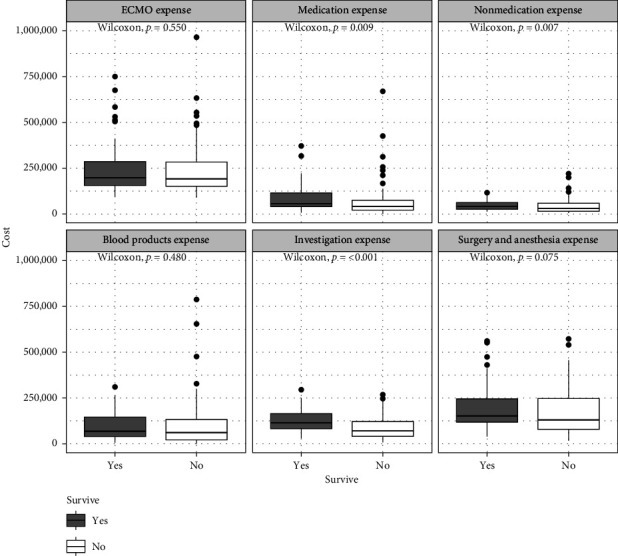
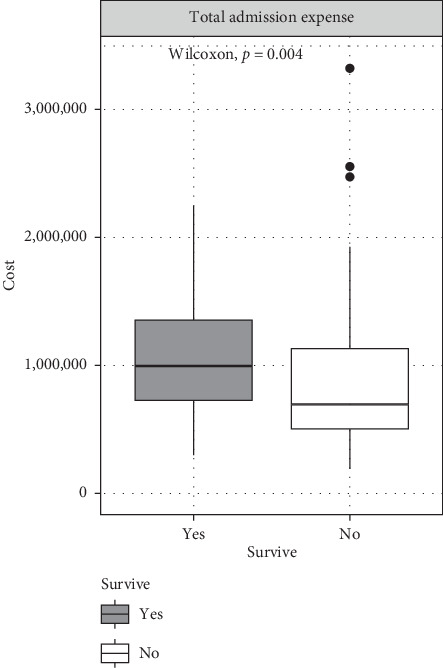
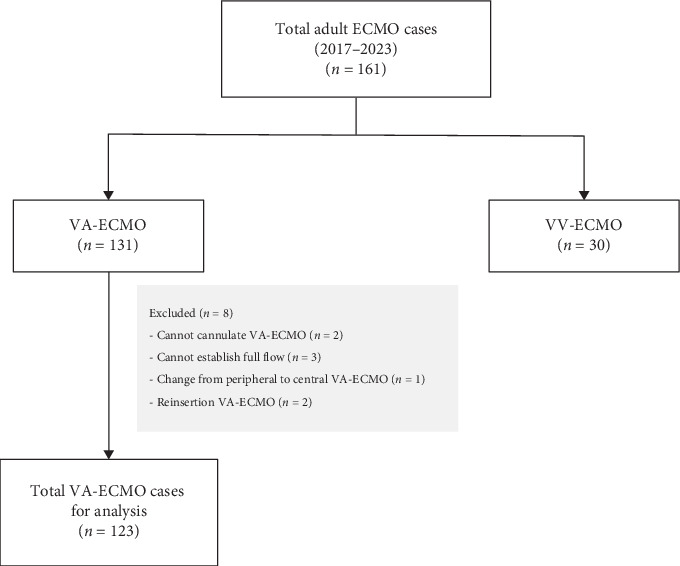
Purpose: Venoarterial extracorporeal membrane oxygenation (VA-ECMO) is a life-saving intervention for refractory cardiopulmonary failure. Identifying factors associated with survival is essential for optimizing patient selection and management. In this study, we aimed to identify VA-ECMO survival predictors and evaluate the associated complications, costs, and outcomes. Methods: A retrospective analysis was conducted on data from 123 adult patients who underwent VA-ECMO at the Songklanagarind Hospital between 2017 and 2023. Clinical characteristics, ECMO-related complications, hospital expenses, and survival outcomes were analyzed. Univariate and multivariate logistic regression analyses were used to determine independent predictors of survival. Results: Fifty (40.7%) patients survived until hospital discharge. Compared to central VA-ECMO, peripheral VA-ECMO was significantly associated with improved survival (adjusted OR: 26.44, 95% CI: 1.95-358.7, p = 0.014). Preexisting liver dysfunction (adjusted OR: 0.27, 95% CI: 0.09-0.79, p = 0.016) and renal dysfunction (adjusted OR: 0.29, 95% CI: 0.1-0.85, p = 0.023) were independent mortality predictors. Survival odds were significantly lower in patients with American Society of Anesthesiologists (ASA) Class 5 (adjusted OR: 0.07, 95% CI: 0.01-0.67, p = 0.022). Neurological complications were more common in nonsurvivors than in survivors (41.1% vs. 18%, p = 0.012). Survivors had significantly higher total hospital costs (997,563.5 vs. 696,191 THB, p = 0.004) and longer hospital stays (28.5 vs. 3 days, p < 0.001). The multivariate model demonstrated strong predictive performance, with an area under the curve of 0.85. Conclusions: ECMO cannulation strategy, preexisting liver and renal dysfunction, and ASA classification were key factors associated with survival. Peripheral VA-ECMO was associated with better outcomes, and organ dysfunction significantly increased the mortality risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


