Serum Alpha-Fetoprotein-Tumor Size Ratio as a Prognostic Marker After Hepatic Resection for Primary Hepatocellular Carcinoma: Propensity Score Matched Retrospective Cohort Study.
Shutian Mo, Yongfei He, Tianyi Liang, Guangzhi Zhu, Hao Su, Chuangye Han, Tao Peng
{"title":"Serum Alpha-Fetoprotein-Tumor Size Ratio as a Prognostic Marker After Hepatic Resection for Primary Hepatocellular Carcinoma: Propensity Score Matched Retrospective Cohort Study.","authors":"Shutian Mo, Yongfei He, Tianyi Liang, Guangzhi Zhu, Hao Su, Chuangye Han, Tao Peng","doi":"10.2196/64929","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with hepatocellular carcinoma (HCC) exhibit a high rate of recurrence and poor prognosis after surgery, and effective prognostic indicators and stratification strategies are currently lacking. Hence, this study proposes new prognostic markers to provide a theoretical basis for patients with HCC.</p><p><strong>Objective: </strong>We aim to build and evaluate a model estimating the effect of alpha-fetoprotein-tumor size ratio (ATR) on the prognosis of patients undergoing hepatectomy for HCC.</p><p><strong>Methods: </strong>We retrospectively reviewed hospital records to identify patients who underwent hepatectomy for HCC at the First Affiliated Hospital of Guangxi Medical University from January 2013 to December 2018. Outcomes (recurrence events and mortality) not available in the outpatient medical records were determined through telephone interviews until February 2022. The optimal cutoff value was determined using X-tile (Yale School of Medicine). Independent risk factors for prognosis were investigated by Cox regression modeling, and between-group differences were reduced through propensity score matching. A predictive model for HCC prognosis was constructed using a nomogram, and the predictive performance of the model was evaluated using the C-index.</p><p><strong>Results: </strong>Of the 1628 eligible patients, 1204 patients were included in the analysis. Patients were stratified into low, medium, and high ATR groups with X-tile. Before propensity score matching, ATR was identified as an independent risk factor for overall survival (low vs medium: HR 1.41, 95% CI 1.03-1.94; P=.03; medium versus high: HR 1.59, 95% CI 1.02-2.47; P=.04) and relapse-free survival (low vs medium: HR 1.33, 95% CI 1.03-1.70; P=.03; medium versus high: HR 2.10, 95% CI 1.40-3.15; P<.001) of patients with HCC following hepatectomy. A nomogram incorporating ATR, China Clinic Liver Cancer staging, bleeding, and postoperative transcatheter arterial chemoembolization was developed to predict moderate predictive efficacy for overall survival (C-index: 0.73) and relapse-free survival (C-index: 0.73). ATR was found to be associated with microvascular, macroinvasion, and poor tumor differentiation.</p><p><strong>Conclusions: </strong>ATR is an independent prognostic risk factor in patients with HCC after hepatectomy and is associated with microvascular, macroinvasion, and poor tumor differentiation.</p>","PeriodicalId":45538,"journal":{"name":"JMIR Cancer","volume":"11 ","pages":"e64929"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12380365/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/64929","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients with hepatocellular carcinoma (HCC) exhibit a high rate of recurrence and poor prognosis after surgery, and effective prognostic indicators and stratification strategies are currently lacking. Hence, this study proposes new prognostic markers to provide a theoretical basis for patients with HCC.
Objective: We aim to build and evaluate a model estimating the effect of alpha-fetoprotein-tumor size ratio (ATR) on the prognosis of patients undergoing hepatectomy for HCC.
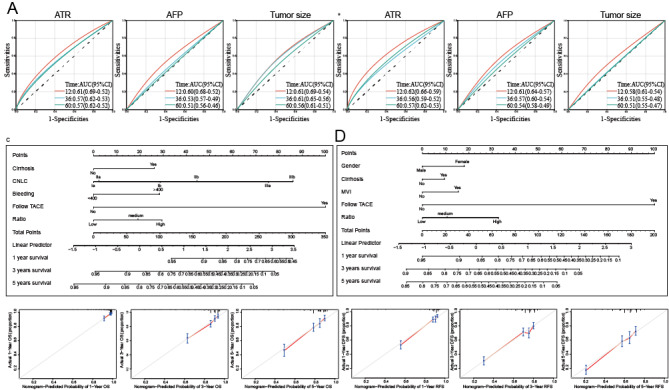
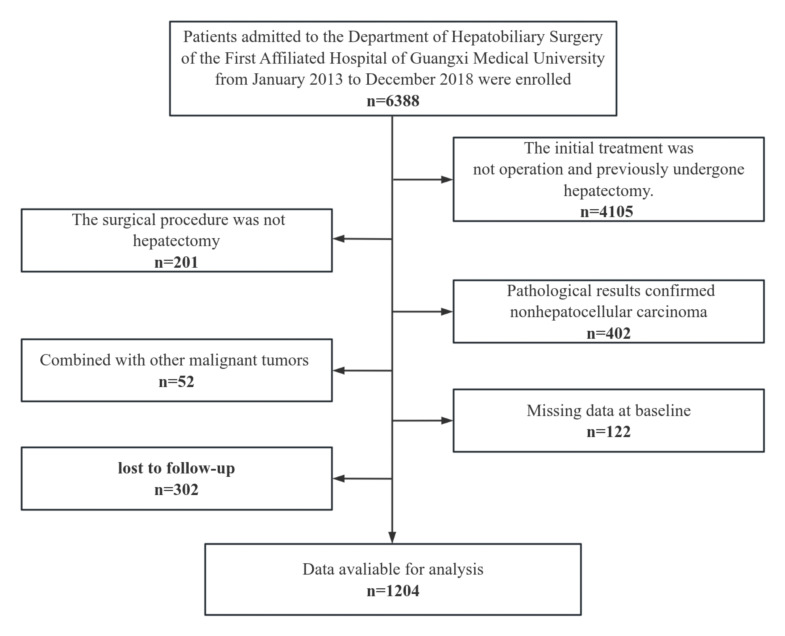
Methods: We retrospectively reviewed hospital records to identify patients who underwent hepatectomy for HCC at the First Affiliated Hospital of Guangxi Medical University from January 2013 to December 2018. Outcomes (recurrence events and mortality) not available in the outpatient medical records were determined through telephone interviews until February 2022. The optimal cutoff value was determined using X-tile (Yale School of Medicine). Independent risk factors for prognosis were investigated by Cox regression modeling, and between-group differences were reduced through propensity score matching. A predictive model for HCC prognosis was constructed using a nomogram, and the predictive performance of the model was evaluated using the C-index.
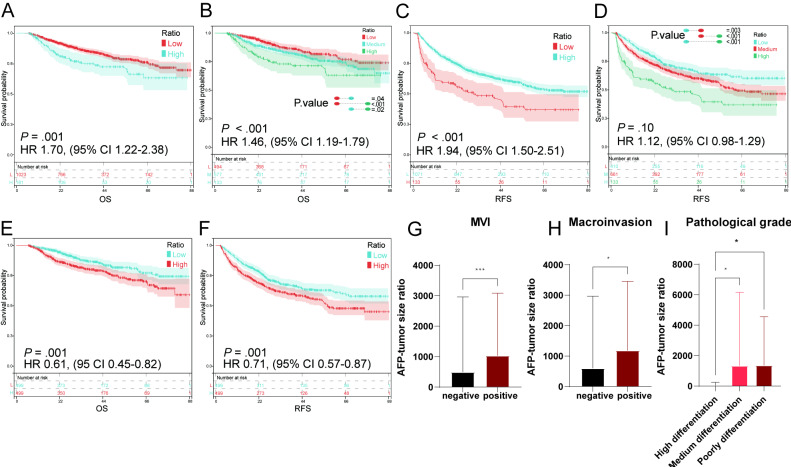
Results: Of the 1628 eligible patients, 1204 patients were included in the analysis. Patients were stratified into low, medium, and high ATR groups with X-tile. Before propensity score matching, ATR was identified as an independent risk factor for overall survival (low vs medium: HR 1.41, 95% CI 1.03-1.94; P=.03; medium versus high: HR 1.59, 95% CI 1.02-2.47; P=.04) and relapse-free survival (low vs medium: HR 1.33, 95% CI 1.03-1.70; P=.03; medium versus high: HR 2.10, 95% CI 1.40-3.15; P<.001) of patients with HCC following hepatectomy. A nomogram incorporating ATR, China Clinic Liver Cancer staging, bleeding, and postoperative transcatheter arterial chemoembolization was developed to predict moderate predictive efficacy for overall survival (C-index: 0.73) and relapse-free survival (C-index: 0.73). ATR was found to be associated with microvascular, macroinvasion, and poor tumor differentiation.
Conclusions: ATR is an independent prognostic risk factor in patients with HCC after hepatectomy and is associated with microvascular, macroinvasion, and poor tumor differentiation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


