Mutita Siriruchatanon, Emily R Brooks, Alexander R Kerr, Denise M Laronde, Miriam P Rosin, Stella K Kang
{"title":"Simulation Modeling of Oral Cancer Development with Risk Stratification: How Potential Screening Programs Can Be Evaluated.","authors":"Mutita Siriruchatanon, Emily R Brooks, Alexander R Kerr, Denise M Laronde, Miriam P Rosin, Stella K Kang","doi":"10.1177/23814683251353226","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background.</b> A barrier to early-stage oral cavity cancer detection is the lack of a defined population and screening regimen satisfying risk-benefit considerations. <b>Methods.</b> We constructed a microsimulation model, Simulation of Cancers of the Oral cavity and Risk Exposures (SCORE), that incorporates risk profiles defined by smoking and alcohol exposure. SCORE simulates the development and progression of oral potentially malignant disorders (OPMD) representing benign, dysplastic, or malignant lesions in the US population starting at age 40 y. OPMD high-risk characteristics of malignant transformation informed a biopsy decision rule. SCORE was calibrated to national cancer registry data. We compared life expectancy in those aged 40 to 60 y with OPMDs, cancer incidence, and cancer-specific deaths across screening strategies with and without the biopsy decision rule, assuming screening every 3 y starting at age 50 y. <b>Results.</b> In US men, all screening strategies reduced cancer incidence and cancer-specific mortality by at least 26% and 20% compared with no screening. Whether with or without a biopsy decision rule, life expectancy among those aged 40 to 60 y with OPMDs was 36.37 ± 0.01 life-years, a gain of 0.03 life-years. However, the use of the biopsy rule improved diagnostic efficiency with 8 biopsies per treatable diagnosis. Screening with or without the biopsy decision rule in high-risk men demonstrated comparable benefit, reducing cancer-specific deaths by 27% and incidence by 20% compared with no screening. Meanwhile, in the non-high-risk subpopulation, applying the biopsy rule avoided the harms of excess procedures, reducing lifetime biopsies by 38% versus biopsy of all OPMDs while preserving reductions in cancer burden. <b>Conclusions.</b> SCORE enables virtual trials of various screening regimens and target populations. Given the time and cost of clinical trials, SCORE may facilitate the evaluation of new technologies and clinical recommendations.</p><p><strong>Highlights: </strong>A new oral cancer simulation model with risk factors including degrees of smoking and alcohol exposure, oral lesion features, and sex incorporates more accurate and precise representation of patient risk categories.We evaluated screening strategies for oral potentially malignant disorders with or without risk-stratified biopsy referral in both the general population and subpopulations defined by degrees of smoking and alcohol exposure.Men with a high degree of both smoking and alcohol exposure exhibited a significant reduction in cancer-specific deaths and cancer incidence from screening programs for oral potentially malignant disorders.Screening with risk-stratified biopsy, using a surgical treatment threshold of moderate dysplasia or worse, yielded the greatest efficiency in term of biopsies needed to detect 1 treatable case.</p>","PeriodicalId":36567,"journal":{"name":"MDM Policy and Practice","volume":"10 2","pages":"23814683251353226"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12368318/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23814683251353226","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
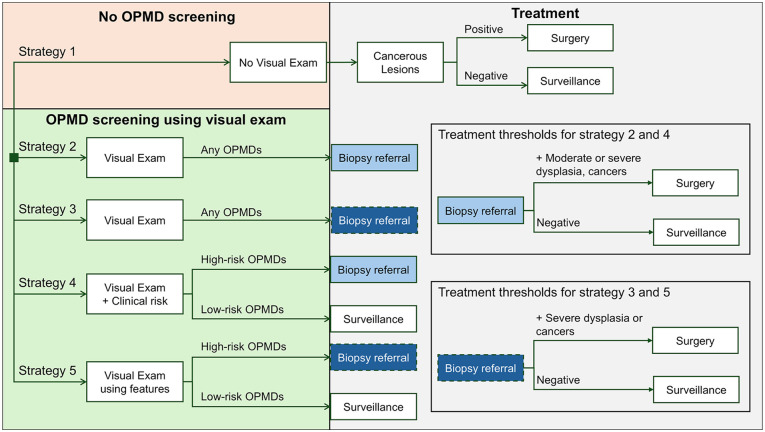
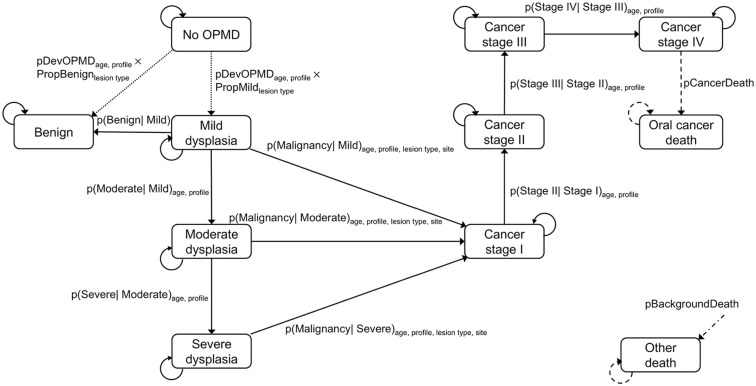
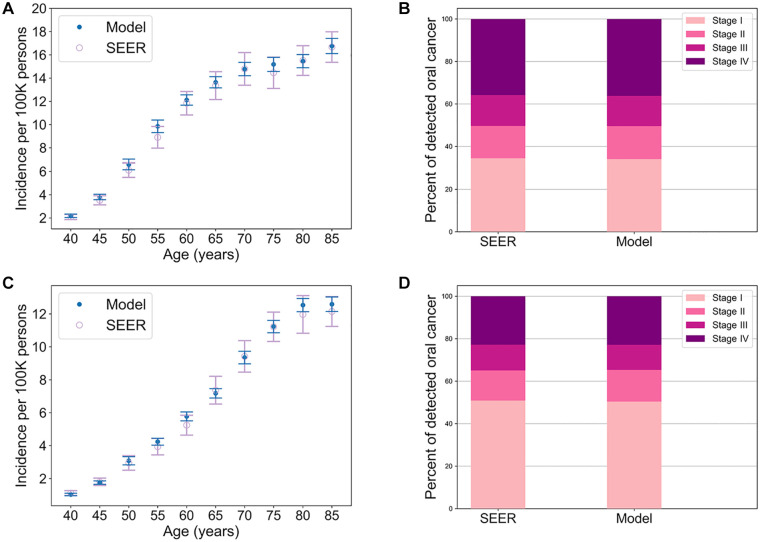
Background. A barrier to early-stage oral cavity cancer detection is the lack of a defined population and screening regimen satisfying risk-benefit considerations. Methods. We constructed a microsimulation model, Simulation of Cancers of the Oral cavity and Risk Exposures (SCORE), that incorporates risk profiles defined by smoking and alcohol exposure. SCORE simulates the development and progression of oral potentially malignant disorders (OPMD) representing benign, dysplastic, or malignant lesions in the US population starting at age 40 y. OPMD high-risk characteristics of malignant transformation informed a biopsy decision rule. SCORE was calibrated to national cancer registry data. We compared life expectancy in those aged 40 to 60 y with OPMDs, cancer incidence, and cancer-specific deaths across screening strategies with and without the biopsy decision rule, assuming screening every 3 y starting at age 50 y. Results. In US men, all screening strategies reduced cancer incidence and cancer-specific mortality by at least 26% and 20% compared with no screening. Whether with or without a biopsy decision rule, life expectancy among those aged 40 to 60 y with OPMDs was 36.37 ± 0.01 life-years, a gain of 0.03 life-years. However, the use of the biopsy rule improved diagnostic efficiency with 8 biopsies per treatable diagnosis. Screening with or without the biopsy decision rule in high-risk men demonstrated comparable benefit, reducing cancer-specific deaths by 27% and incidence by 20% compared with no screening. Meanwhile, in the non-high-risk subpopulation, applying the biopsy rule avoided the harms of excess procedures, reducing lifetime biopsies by 38% versus biopsy of all OPMDs while preserving reductions in cancer burden. Conclusions. SCORE enables virtual trials of various screening regimens and target populations. Given the time and cost of clinical trials, SCORE may facilitate the evaluation of new technologies and clinical recommendations.
Highlights: A new oral cancer simulation model with risk factors including degrees of smoking and alcohol exposure, oral lesion features, and sex incorporates more accurate and precise representation of patient risk categories.We evaluated screening strategies for oral potentially malignant disorders with or without risk-stratified biopsy referral in both the general population and subpopulations defined by degrees of smoking and alcohol exposure.Men with a high degree of both smoking and alcohol exposure exhibited a significant reduction in cancer-specific deaths and cancer incidence from screening programs for oral potentially malignant disorders.Screening with risk-stratified biopsy, using a surgical treatment threshold of moderate dysplasia or worse, yielded the greatest efficiency in term of biopsies needed to detect 1 treatable case.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


